
Dr. Meza, closing the chest
I apologize for the wordiness of this post – but much of what we discuss below is covered in the Bogotá, Cartagena and Mexicali books – the essential mechanisms of cardiac surgery; how procedures work, what is off-pump surgery, when do we use the bypass pump and other explanatory information. But since I have am not writing a full book on Medellin, I wanted to offer a bit of a primer for my new internet readers here.
Dr. Luis Meza
Cardiac surgeon, Hospital General de Medellin
After interviewing Dr. Meza and meeting many of the staff at Hospital General de Medellin, it was a pleasure to be invited to observe Dr. Meza and Dr. Urequi , the head of the cardiac surgery department in the operating room. Despite the patient’s young age, the surgery (for me as an observer) was knuckle-biting. While the surgery itself was a fast, straight-forward and uncomplicated repair of an interauricular septal defect – it was the patient’s fragile condition that had me on the edge of my seat.
Complex patients The case was typical of many of the cases they see at public hospitals. It was a young patient with newly diagnosed right-sided heart failure due to an uncorrected congenital defect. The patient had traveled from another part of Colombia (one of the poorer regions) to have surgery. The patient had initially presented to a local doctor after a syncopal event (passing out) and was found to have an enlarged heart, with a moderate sized pericardial effusion (fluid in the sac around the heart.) After arriving at HGM, the patient was also diagnosed with a serious acquired coagulopathy (bleeding disorder).

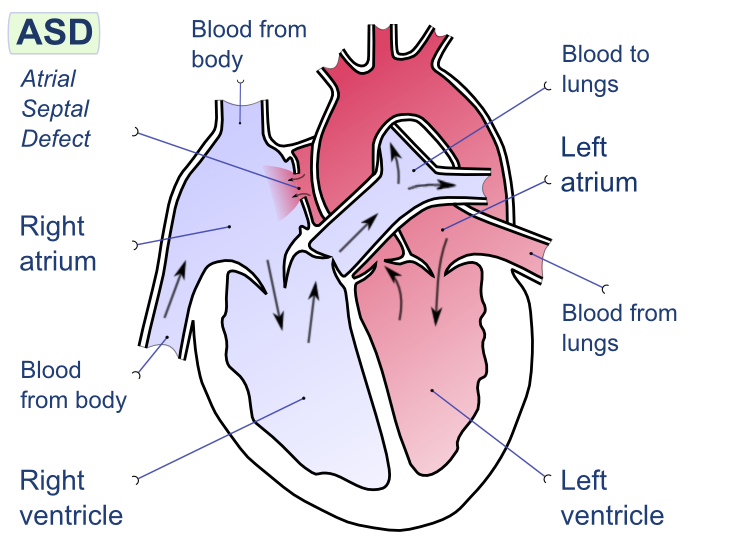
drawing courtesy of Wikipedia (Creative Commons licensing)
Since the patient had a hole between the left atrium leading into the right atrium, blood was being pushed from the left atrium (which is under higher pressure) to the low pressure right atrium. Over the course of many years, this had caused the right atrium to enlarge massively. As the right atrium was continuously being overfilled (from blood from the left side), the right side of the heart was being forced to work harder, and harder. As the atrium continued to be overstretched, and enlarged – it also caused blood to be forced back into the pulmonary arteries – causing pulmonary hypertension. While pre-surgical tests (echocardiogram, and cardiac catheterization) showed the patient to have (only) moderate pulmonary hypertension (with PA systolic pressures of 65mmHg).
Pre-operative testing is only part of the story
However, when we looked down, into the patient’s chest – it was obvious that the patient’s pulmonary vasculature was engorged and enlarged. The patient’s heart was massive, and floppy (which is a sign the heart is working way too hard). The patient also had peripheral edema which is another sign that the heart was not working well.
Potential for badness*
So even though, the surgery itself (described below) is not terribly technically challenging (‘like darning socks’ one surgeon used to say) – a lot can go wrong because the patient’s heart just doesn’t work that well to begin with.
* a not-so-scientific term to describe the likelihood of potential complications, problems or adverse outcomes. These may be unavoidable circumstances in many cases – but the term is a reminder to remain vigilant even during so-called “simple” procedures.
Nitric oxide on hand
This OR does have nitric oxide – (which we didn’t need), but was available nearby, just in case. Nitric oxide, milrinone and other medications are critical to have on hand in patients with pulmonary hypertension. Some patients will never need it – others can’t survive without it – and sadly, (in patients with severe fixed pulmonary hypertension), nothing – not even an assist device is going to make much difference. While we can try to predict which patients are going to tolerate surgery, it’s not always clear-cut. Tests (echocardiograms, right heart caths) can predict, tests can give probabilities – but sometimes tests are wrong, and patients who appear to have only ‘mild’ disease do very poorly (and visa versa). Sometimes, we just have to hold our breath as the patient comes off bypass and see.

canisters of nitric oxide in OR #1
As I mentioned in a previous post – cardiac surgery procedures can be a bit more complicated than many other surgical procedures, and while having something like nitric oxide on hand doesn’t seem like a big deal – it is. (I have worked in several facilities without these capabilities). It also speaks to the general preparedness of the staff. But despite the ‘potential for badness’ everything proceeded beautifully with Drs. Urequi and Meza. The case seemed to speed by despite the patient’s fragile health. The entire CPB (cardiopulmonary bypass run) was just 26 minutes with a total cross-clamp time of 31 minutes.)
A little bit about cardiopulmonary bypass – the “heart-lung machine”
In comparison to the congenital repair above, average CPB times for valve replacement run around 100 minutes, 60 to 90 minutes for bypass surgery. Patients have a higher risk of CPB related complications from hypo/ altered perfusion after long pump runs . As the clock begins to exceed 120 minutes, the risk of renal failure, cognitive changes and bleeding problems (as blood cells are continuous smashed/ broken / damaged within the pump) increase.

Perfusionist operating bypass pump aka “heart-lung machine”
What is “Off-pump surgery”? Nowadays, lots of people get real excited about “off-pump” surgery because they think that by not using the heart-lung machine, they can avoid a lot of the problems we mentioned above. But that’s oversimplifying the entire scenario – and one that I find is often used to “sell” a particular surgeon or surgical program. Off-pump can be safer than CPB cases, for some patients. But these are usually not the patients that the surgery is sold to.. So it’s important to know what some of the terminology really means. Just because Hospital X has billboards announcing that they now perform off pump surgery – doesn’t mean that it’s something you may even need or want.
Off pump is not for everyone
Patients have to be fairly healthy to tolerate cardiac surgery without the pump. People with a lot of the problems that we thought were worsened by the pump, actually fare worse when we try to do surgery without the heart-lung machine. For example, we initially thought that Off-pump surgery would be great for people with renal insufficiency or ‘bad kidneys’ – particularly people who have kidney problems but aren’t quite sick enough to be on dialysis yet. The hope was that by avoiding the bypass pump we could avoid any damage to the kidneys from artificial flow/hypoperfusion because one of the biggest risks of cardiac surgery in patients with bad kidneys is that surgery will cause their kidneys to fail entirely, and make patients dialysis dependent. Unfortunately, the research from all of the off-pump surgeries being done hasn’t really shown the benefits that we thought it would. So like most things in medicine, it’s not quite the panacea we had hoped it was. But we did learn an incredible amount of information once surgeons started trying off pump surgeries for coronary bypass. Surprisingly, we learned that many of the complications, and conditions that we had long blamed on the CPB pump – weren’t related to the machine at all. But much of this is still being argued by cardiac surgeons every single day – each with different research studies giving different results..
More importantly, Off-pump not possible for many types of cardiac surgery
It’s technically impossible to do some types of cases without the bypass pump. Coronary bypass surgery (CABG) is very different from other types of surgery, for example. During bypass, the surgeon is only operating on the outside of the heart – attaching new conduit (arteries and veins) to arteries on the surface of the heart. So – it isn’t absolutely essential to have the pump circulating blood for him while he’s operating – in some patients – we can let their body do it for us during surgery.
But replacing diseased heart valves, or the great vessels (aortic aneurysms etc) is a completely different entity. In those surgeries – the surgeon is cutting into the heart or great vessels themselves. It’s not possible to lop off the top of the aorta, operate on the aortic valve and not have blood being re-directed mechanically during this process. Otherwise blood would just literally spill out into the chest and never oxygenate the brain and the rest of the body. (The only time we ever do this kind of procedure without a pump is during organ retrieval – for obvious reasons). It’s important to know these distinctions so people understand how the surgery actually proceeds.
For the case today – the surgeon has to make an incision through the side of the atria (wall of the heart chamber) to get to the hole on the inside wall of the heart.) The surgeon then closes the hole with suture (and a patch, in some cases). Some doctors do this in the cath lab without surgery – but that’s also controversal because the patch used in the cath procedures in the past has caused a high incidence of stroke. In a young patient like the one here – you certainly wouldn’t want to risk it – particularly since we don’t know how well those patches hold up in the long term.

- Cardiac surgeons operate at Hospital General de Medellin (HGM)
Overall evaluation of today’s case:
Safety checklists, and all pre-operative procedures were completed. Patient was prepped and draped in an appropriate sterile fashion. Antibiotics were administered within the recommended window (of time). Appropriate records were maintained during the case.
Surgery proceeded normally and without incident.
Due to an underlying coagulopathy the patient did require administration of nonautologous blood products (4 units of packed red blood cells, 3 packets of platelets, and abumin) while on pump. While the facility does not have a ‘cell-saver’ for washing and re-infusing shed blood, patient did receive autologous(their own) transfusion from the CPB pump. This blood, from the CPB circuit was returned to the patient to limit the amount of blood needed after surgery. Hemoglobin at the conclusion of surgery was 9.6mg/dl, which is within acceptable parameters.
Hemostasis was obtained prior to chest closure, with only a small amount of chest tube drainage in the collection chamber at the time of transfer to the intensive care unit.
Surgical Apgars – do not apply for cardiac cases due to the nature of the case, and use of CPB. Mean pressure while on CPB was within an acceptable range. Patient’s urinary output was less than anticipated during the case (150cc) despite the use of mannitol while on pump, but the patient responded well (1000+) with volume infusion and the addition of furosemide.
The patient was hemodynamically stable during the entire case. The was a very brief transitory period of hypotension (less than 5 minutes) near the conclusion of the case, which was immediately noted by anesthesia and treated with no recurrence.
On transfer to the unit, the patient was accompanied by several members of the OR staff, including Dr. Meza, the anesthesiologist, and the perfusionist, each of which did a face-to-face “hand-off” report of the patient (and medical history) including the course of the surgical procedure (including medications given, lab values, procedural details) to the Intensivist (physician), with ICU nursing staff attending to the patient.
Transesophageal echo (TEE) was not performed during this case, but was available if needed.
Also, I am happy to report there were no smartphones or “facebooking” in sight. No one appeared engaged in anything other than the surgery at hand.



















































{kind=link}