Tuesday – We drove back from Cartagena this morning before heading to surgery in the afternoon for a bypass grafting case. For the first half of the way, I sat in the back and enjoyed looking out the window. It’s amazing how dry parts of Bolivar are.
The drought has been responsible for the deaths of over 20,000 farm animals here in Colombia. The small lakes are disappearing, from my first trip to Sincelejo to my most recent visit just a few weeks later. The trees and bushes besides the roadways are completely coated with layers of dust from passing vehicles. It gets greener as we pass into Sucre, but it’s a sad reminder of the devastating effects of climate change.
After stopping for breakfast along the way, where we met up with Dr. Melano, Iris went with Dr. Melano and I stayed with Dr. Barbosa. We talked about music mostly. At one point, a former patient from several years ago called, just to say hello. The patient had recently heard that Dr. Barbosa now had a surgery program in Sucre. (The patient had previously traveled to Cartagena from a small town in Sucre for surgery.)
Once we got to Sincelejo, we headed to the hospital to see our patient before surgery and go over any last-minute questions or concerns.
(Of course) I was worried about finding vein but we easily found good quality conduit. Dr. Salgua has been very nice about helping me with the saphenectomies. The team teases me because I have a difficult time pronouncing her name. We have a kind of system: While I finish closing the leg, she moves up the table to assist the surgeon in starting the grafts. Then when I finish wrapping the leg, I stay at the back of the table with the instrumentadora, learning the Spanish names for all the instruments. Once the chest is closed, she does a layer of fascia and I close the skin incision.
It’s a little crowded sometimes with the new instrumentadora learning the essentials of cardiac surgery, but the atmosphere at the back of the table is a lot different from the climate at the top. (Dr. B is always calm, pleasant and entertaining – but Dr. Salgua is almost completely silent the whole time). I am a lot quieter than my “out of OR self” when I am across the table from the surgeon too..
Wednesday – Another coronary case, on a fragile-ish patient (multiple co-morbidities including chronic kidney disease etc). It was a long case and I was a little worried the whole time but the patient did well. (I always worry about the frail patients).
I did okay too – performing a saphenectomy with Dr. Barbosa. The patient had a vein stripping procedure previously (on one leg only) so I wanted to be sure to get a good segment of vein on the remaining vein. I think Dr. Barbosa was worried about the quality of the conduit (because he kind of hovered – and didn’t relax until we started harvesting it.)
Skip harvesting
I wish I would have more opportunities to perform a traditional saphenectomy (one very long incision). I assisted on one several years ago – and I think if I had a chance to do a couple more, I would feel more comfortable skip harvesting. Of course, a headlamp would also help. (It’s kind of dark looking down the skip ‘tunnels’). Then once I’ve mastered skip harvesting, I think it’s just another small jump to endo-harvesting with a scope. I know a lot of people never bother learn to skip harvest, but I feel more comfortable building on the principles of open procedures first. I might need them in an emergency case which is kind of why I wished I had more open saphenectomy experience.
Thursday – Saw three patients in the clinic today. However, on reviewing the patient records and an intra-office echocardiogram, one of the patients definitely doesn’t need surgery at this point. (Asymptomatic with only moderate valvular disease). We were happy to let him know he didn’t need surgery even if that means fewer cases.
Two surgeries today. The first case was a bypass case for a patient with severe coronary disease and unstable angina. Dr. Salgua and I did the harvest. I think Dr. Barbosa is a little nervous about handing over the reins to me for harvest because he keeps a pretty close eye on me while I am doing it. But then again, it might be because I am a little overly cautious and hesitant at this point. If I didn’t have Dr. Salgua to look over my shoulder and encourage me onward, I’d put clips on everything and proceed at a snail’s pace to make sure I do it right. But since it’s still my first week, maybe I shouldn’t be so hard on myself.
On the other hand, he must think my suturing is pretty good, because he just trusts me to do it correctly.
The second case was a patient from last week, who developed a large (symptomatic) pleural effusion and cardiac effusion (no tamponade or hemodynamic instability) which is a pretty common surgical complication. The case proceeded well – I placed the chest tube, with Dr. Barbosa supervising. Dr. Barbosa performed the cardiac window portion of the procedure.
Sadly, one of our patients from last week died today. It was a fragile patient to begin with, and even though surgery proceeded well, the patient could never tolerate extubation and had to be re-intubated twice after initially doing well. From there, the patient continued to deteriorate.
Friday
Today we had a beautiful aortic valve surgery. This has always been one of my favorite cardiac procedures. Somehow its elegant in the way the new valve slides down the carefully coördinated sutures. (I don’t have pictures from this case – since I was first assisting – but I will post some from a previous case – so you can see what I mean).
Dr. Salgua worked an overnight shift, so I was at the top of the table – (and yes, noticeably quieter than normal.) I was surprised at how fast it seemed to go – but maybe that’s because everything went so smoothly. Or maybe because we’ve done a lot of coronaries lately, which is a much more tedious and time-consuming process.
Iris and I are working on a patient education process – as a way to improve the continuum of care for patients (particularly after discharge). I really enjoy working with Iris because I feel like we are always on the same page when it comes to patient care.
While it’s been a tiring week for the crew – I am, as always! exhilarated and happy to be here in Sincelejo. Just knowing it’s the end of another week (and I am that much closer to going home) has me feeling a little sad. But I guess I can’t stay forever, and I sure don’t want to take advantage of all the kindnesses that have been extended to me.
That being said:
At the end of every surgery, every day and every week in Sincelejo – I am grateful. Grateful to Dr. Barbosa for being such a willing and patient teacher – grateful to the operating room crew (especially Iris Castro and Dr. Salgua) and particularly grateful to all the kind and generous patients I have met and helped take care of*.
The medical mission
This week I had another inquiry about ‘medical missions’. I know people mean well when they ask about medical missions, or when they participate in these types of activities but…
Long time readers know my philosophy on this – don’t go overseas so you can pat yourself on the back over the ‘great deeds’ you performed ‘helping the poor’. It’s patronizing to the destination country and its inhabitants – and generally not very useful anyway. An awful lot of volunteers with real skills and talents go to waste on these so-called mission trips when their skills might be better served (in less exciting or glamorous ways) in free clinics in our own country.
But it does give everyone involved a chance to brag about how selfless and noble they have been; traveling thousands of miles, sleeping somewhere without 24/7 wi-fi (and who knows what other hardships).
Instead, change your orientation – and maybe challenge that assumption that everything you’ve learned about medicine, health care and taking care of people is better and superior. Open your eyes and be willing to learn what others have to teach you instead.
* I always opt for full disclosure and transparency with the patients. I introduce myself and explain that I am a studying with Dr. Barbosa, what my credentials and experience is to give them the opportunity to ‘opt out’.
Here in Cartagena, I have been fortunate enough to have two great roommates; Iris and Ximena.
Dr. Barbosa made all the arrangements for me, and I was a little nervous about bunking down with another nurse (we can be temperamental and territorial at times) but living with Iris has been absolutely wonderful.
I was kind of worried I’d be living with some young, possibly flighty nurse who might resent having a middle-age woman in her home, cramping her style. Instead, it’s like having an instant best friend and I love it.
For starters – we have a lot in common: we are both academically and professionally inclined. Iris is the perfusionist for Dr. Barbosa’s cardiac surgery service and is extremely knowledgeable.
Part of the machinery that makes up Iriis’ professional life: the heart-lung machine
(In Colombia, Perfusion is an advanced nursing degree. Iris obtained her master’s degrees in both critical care (National University) and Perfusion at (CES.). She is widely acknowledged as one of the best perfusionists (if not the best) in all of Colombia. Her peers frequently consult her seeking advice for a variety of surgical circumstances.
She is the only nurse to collaborate (and be listed on the cover) of a comprehensive Colombian textbook on Cardiology. Her name is listed along side such esteemed Colombian physicians as Pablo Guerra, Nestor Sandoval and Sergio Franco.
She also serves as a reviewing editor of several Colombian medical journals. Research articles are sent to Iris to review the methodology/ study design and overall quality. Articles she rejects will not be accepted for publication.
In her free time, it’s not unusual to find her reading the latest journal articles on cardiac surgery or working on presentations for the latest meeting or international conference on perfusion. In fact, she recently returned from the annual Colombian conference on cardiology and cardiac surgery in Medellin. She is equally enthusiastic about all aspects of nursing and the position and rights of women (nurses) in Colombia and in medical society in general.
She is particularly outspoken against much of the machismo that dominates life here. She is the one person I have learned to expect to never ask me the unpleasantly intrusive questions that seem to pass for almost introductory conversation here such as “Why don’t you have children? Don’t you want them? What does your husband think of that? Your husband permits you to be here [in Colombia] without him?”*
Even when we don’t agree on all issues, she never judges my opinions or thoughts. She endeavors to understand my reasoning instead. It’s refreshing.
This combination of intellect, insight and experience makes for a lot of interesting and engaging discussions in the evenings as we relax and enjoy the fragrant breezes that bring daily relief to the sweltering city.
A strong woman in a culture of machismo
Iris is also extremely forthright and independent (traits that also resonate with me.) She takes no ‘guff’ from anyone and lives how she pleases in a society that has a lot of difficulty accepting that (unmarried, no kids with Ximena as a part-time roommate.)
Even my professor, as charming and intelligent as he is, defaults into this kind of ‘macho’ thinking. He tells me he worries about Iris, as “she is all alone” without a man to protect her. He worries she is missing out on true happiness and is destined to be sad, alone. Nothing could be further from the truth.
Rather, Iris has chosen to defy tradition, and live life on her terms. She has friends, family and romantic attachments like anyone else. She just maintains both her privacy and her independence despite that, sort of like Elizabeth I of England.
It is sometimes hard as an outsider to understand why this attracts some much attention – a single woman living quietly in her own apartment. But then I think back to some of the comments I get from friends, acquaintances, co-workers and even strangers regarding locums life, and I realize, that as female professionals; whether the United States or Colombia, we still have a long way to go.
It’s just that as an American, I think I have fallen for the illusion of the possibility of female equality in way that women in other countries never have. (The irony is that at this moment in my home country, women’s rights; to reproductive, financial and professional freedom are being eroded more that any other time in recent history. Hard won battles of the 60’s and 70’s are being erased with nary an outcry.)
Here ‘paternalism’ rules the day – and no one pretends any different.
But there is more to Iris that a forthright, intelligent, independent individual. She is also a nurturer, a caregiver, a nurse in the very sense of the word.
What could be more nurturing that offering up her home to an unknown stranger from another land?
“Ximena”
Iris and the other members of her apartment complex have adopted a white and orange stray cat that answers to a variety of affectionate terms. One of these is “Nena”. One my first day here, I confused “Nena” as a shortened version of Ximena, so Ximena she is.
This straggly looking, mangy little ball of fluff is adored by the residents of the small apartment building. Typical of most cats, she is “owned” by none, but owns each neighbor in turn. But it was Iris who took up donations to get Ximena surgery she needed and routine veterinary care. All the residents share in the feeding and care of the street cat – including applying a cream to her healing surgical scar, but it is Iris whom Ximena usually seeks.
While most of the residents leave their doors open during the afternoons to invite Ximena in, Ximena is most often found either inside our apartment, or bellowing outside the door (on the rare occasions that is is closed.) She wanders in with the grace and arrogance that only a cat possesses.
She carries herself with a dignity that belies her ‘homeless’ state as to say she isn’t a vagabond but a seasoned traveler as she visits each apartment in turn – but always comes back to Iris to stay all afternoon and overnight.
Some of the neighbors our jealous of Ximena’s attention, but with our weekly journeys to Sincelejo, they always have an apportunity to host ‘Nena as their favored guest.
Iris loves to cook – and does so easily, deliciously. She embraces a healthy lifestyle filled with daily exercise and fresh fruit and vegetables.
salad made of exotic fruits
We talk about my love of Colombian food – and together one day in the kitchen, we make brevas. She tells me with a smile that she has never made them, but used to watch her grandmother cook them for a sweet tweet.
Boiling brevas: Photo by Camila
We savor the sugary treat, one breva at a time over the next several days.
In addition to learning how to perform saphenectomies from Dr. Barbosa, Iris is teaching me how to crochet. My first project will be one of the small bags that is in a style typical for Colombia. I think it is ironic that it seems easier to suture that it is to crochet.
But Iris is endlessly patient with me – and slowly, slowly as I unravel my mistakes and start again, I am making progress. She has a blogspot where she showcases her latest creations. She recently received national accreditation as a ‘native artist’ to participate in festivals and art fairs that specialize in traditional Colombia crafts.
Today, as we sit on the sofa, crocheting, we talk about plans for the Semana Santa (Easter Week). The secretarial staff in Sincelejo has vacation plans and wants to keep the office closed all week so she can visit a boyfriend in Medellin – but Iris and I think it should remain open for the patients. We plan to offer to staff the office, so that patients won’t have to wait a week to be seen. We will have to navigate and negotiate carefully and diplomatically to prevent causing any hard feelings but as Iris points out, it’s the right thing to do for the patients – and the doctors, and that’s what matters. (My motives are admittedly more self-serving: more clinic = more surgery.)
*This type of questioning is fairly pervasive throughout Colombia, and is often performed as part of introductory conversation. Once a taxi driver in Bogotá directed me to the nearest fertility clinic when I responded “No” to the question about children. He wasn’t rude, on the contrary, he thought he was being helpful.
If there is such thing as a perfect day, it would have been today. The weather was still hot, humid and sticky. I still have student loans and the world continues to have accidents, disasters and wars. But for me, today was as good as it gets.
I spent the morning in the operating room while Dr. Barbosa performed a septal patch, and repair of the tricuspid valve. The case went well and the patient did beautifully. Before I left the hospital, the patient was already awake, alert and awaiting extubation. There was no hemodynamic instability or bleeding.
The local cardiologist did several cardiac catheterizations today – and we were consulted on four of them. 3 of the patients have excellent targets for bypass grafts and normal heart function. The fourth patient is a little more fragile, but is still a reasonable candidate for surgery.
Best way to see Sincelejo: On the back of a bike*
Lastly, I spent a nice, breezy hour touring the city on the back of a friend’s motorcycle. (Yes, mom – I wore my helmet – and he didn’t drive like a maniac.) We went all over Sincelejo; from the scenic overlook over the valley below, to the football stadium, past the University of the Caribbean, over to a public park with tennis courts, several pools and a small zoo. (I don’t have any pictures because I figured I’d probably drop it).
My guide was Omar, the spouse of my friend, Elena. He works in the Parks & Recreation department of the Sucre.
After returning home, I took a walk down to the Plaza to buy some local cheese. Then I spent the evening eating exotic fruits like guama, plums, uchuvas and fejoas.
Dr. Sergio Franco wrote the book on heart surgery.
It was exciting and illuminating to talk to Dr. Sergio Franco, who is one of Colombia’s most prolific writers and professors of cardiac surgery. The 50 year-old cardiac surgeon has authored multiple textbooks for surgeons and edited ten others, making him one of the nation’s definitive experts on cardiac surgery.
Dr. Franco stands near a collection of his textbooks
Currently he is the Medical Director of the Cardiopulmonary and Peripheral Vascular Center of the Fundacion San Vicente in Rio Negro, as well as Chief of Cardiothoracic Surgery at the Clinica de Medellin. For the last 12 years, he has also been the program director for post-graduate studies at the Universidad CES medical school. Between the two clinics, and the five other surgeons he works with (2 at Clinica de Medellin and 2 at Rionegro), he estimates that the cardiac programs see volumes of 700 – 750 cases per year.
For our first interview, we meet at the Clinica de Medellin to talk. He later invites me to see the hospital at Rionegro.
Education/ Training / Experience
Dr. Franco attended medical school, general surgery residency and cardiac surgery fellowship at the Universidad Pontifica Boliviarana. He finished his fellowship in 1996. As part of his fellowship, he spent nine months training in heart and lung transplantation at Loyola University Medical Center in Chicago, Il. During his heart and lung tranplantation training, he received an award as “Best Foreign Medical Fellow.” He graduated with high honors due to his exemplary grade point average.
He has additional training in thoracic and thoracoabdominal aortic surgery (Missouri Baptist, 1998), and minimally invasive valvular surgery (Cleveland Clinic).
Selected awards and special recognition
He was also the first surgeon to perform endovascular harvesting of the saphenous vein in Colombia in 1997. He received second place for a poster presentation based on this technique at the Colombian Congress of Cardiology and Cardiovascular Surgery, Cartagena, 8 to 11 February 2006.
He received the Cesar Uribe Piedrahita Medal from the Colombian Medical Federation and the Antioquia Medical College in 2003 for academic and clinical excellence, in addition to several other awards for academic achievement.
He was the chapter president of the Colombian Society of Cardiovascular Surgery and the Colombian Surgical Consensus for multiple terms. He was also the Chairman, and Medical Advisory of the first Latin American Forums on cardiovascular surgery.
He has received several awards including “The best of 2006” from Hospital General de Medellin for his assistance in the development, creation and commissioning of the cardiovascular services unit at that facility. He has also presented his work at numerous national and international conferences.
He speaks English in addition to his native Spanish.
Dr Sergio Franco
San Vicente Fundacion
Cardiovascular Surgery
Medical Director, Cardiopulmonary and Vascular Surgery
While I requested a visit to the operating room, an invitation was not forthcoming.
Selected writings of Dr. Sergio Franco
Book chapters:
1. Franco S., Restrepo G. Momento Quirúrgico óptimo en el paciente con enfermedad valvular cardiaca. Libro Tópicos selectos en enfermedades cardiovasculares 2000. Unidad cardiovascular Clínica Medellín. 1 Edición. Página. 101-112. ISBN 958-33-1541-9
2. Franco S. Endocarditis Infecciosa: Visión Quirúrgica – Indicaciones de Cirugía. Libro Tópicos selectos en enfermedades cardiovasculares 2000. Unidad cardiovascular Clínica Medellín. 1 Edición. Páginas 201-211. ISBN 958-33-1541-9
3. Franco, S. Estenosis Mitral – Tratamiento Quirúrgico. En: Franco, S. (Ed) Enfermedad valvular cardiaca. Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 111-116 Abril 2001. ISBN : 958-33-2244-X
4. Franco, S., Giraldo, N. , Vélez JF. Uso e Indicaciones deHomoinjertos – Cirugía de Ross. En: Franco, S (Ed) Enfermedad Valvular Cardiaca. Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 70 – 77, Abril 2001. ISBN : 958-33-2244-X
5. Alzate L., Franco S. Factores hemodinámicos y físicos de las válvulas cardiacas artificiales. En: Franco, S. (Ed) Enfermedad Valvular Cardiaca – Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 222 – 228 Abril 2001. ISBN : 958-33-2244-X
6. Franco, S., Vélez, J. Revascularización Quirúrgica del Miocardio: Estado actual. En: Tópicos selectos en terapéutica cardiaca y vascular 2001. Cardiología Clínica Medellín. P: 108 –120. Primera edición, Octubre 2001. ISBN : 958-33-2607-0
7. Vélez, JF, Franco, S., Tamayo L. Tratamiento quirúrgico de la enfermedad coronaria. En: Enfermedad Coronaria. Pineda M, Matiz H, Rozo R. (Ed), septiembre 2002. Capitulo 36, pgnas 609-630. ISBN : 958-33-3945-8
8. Franco, S.Intervencion Quirúrgica de los síndromes coronarios agudos. En: Tópicos selectos en enfermedades cardiovasculares, 2002. Pgna 177-192 (Velásquez D, Uribe W, editores) Ed. Colina, Departamento de Cardiología Clínica Medellín 2002. ISBN 958-33-3663-7
9. Franco, S.Cardiopatías Congénitas del Adulto. En: Tópicos selectos en cardiología de consultorio 2003. Pgnas 193-211. (Restrepo G., Uribe W., Velásquez D., editores). Ed. Colina, Cardiología Clínica Medellín, 2003. ISBN : 958-33-4858-9
10. Franco, S.Enfermedad Valvular Cardiaca: Indicaciones de Cirugía. En: Libro II Congreso medicina cardiovascular y torácica. . Hospital Departamental Santa Sofía de Caldas, 2003 (Jaramillo O., Editor) Editorial Tizan. Pgnas 87-104
11. Franco, S.Tratamiento Quirúrgico de la Fibrilación Atrial. En: Libro II Congreso medicina cardiovascular y torácica. Hospital Departamental Santa Sofía de Caldas, 2003. (Jaramillo O., Editor) Editorial Tizan. Pgnas 123-131
14. Franco, S., Giraldo, N. Tratamiento Quirúrgico del Paciente Valvular en Falla Cardiaca. En: Enfermedad Valvular Cardiaca. Paginas 169 – 176. (Franco, S., Editor). Editorial Colina. Primera Edición 2004. 227 paginas. ISBN 958-33-6218-2
15. Franco, S. Jiménez A. Factores Físicos y Hemodinámicos de las Prótesis Valvulares Cardiacas. En: Enfermedad Valvular Cardiaca. Pgnas 223-227. (Franco, S., Editor). Editorial Colina. Primera Edición 2004. 227 paginas. ISBN 958-33-6218-2
16. Franco, S.Guías de manejo de las valvulopatias aorticas. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2004. Pgnas 143-149. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2004. 195 paginas. ISBN 958-33-6285-9
17. Franco, S.Guías de manejo de las valvulopatias mitrales. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2004. Pgnas 149-155. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2004. 195 paginas. ISBN 958-33-6285-9
18. Franco, S.Tratamiento Quirúrgico de la Fibrilación Atrial. En: Falla Cardiaca, Diagnostico y manejo Actual. 2004. Pgnas 271- 287.. (Castro, H; Cubides, C. Editores) Editorial Blanecolor, Primera edición, 2004. 431 pgnas. ISBN 33-6689-7
19. Escobar, A. Franco, S. Trauma de grandes vasos torácicos. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 160- 169. 193 paginas. ISBN : 958-33-7698-1
20. Franco, S., Vélez, A. Trauma cardiaco. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 154- 159. ISBN : 958-33-7698-1
21. Franco, S., Jaramillo, J. Tumores cardiacos. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 117 – 123. 193 paginas. ISBN : 958-33-7698-1
22. Franco, S., Vélez, A. Trauma cardiaco. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. Manual Condensado. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 362- 366. 388 paginas. ISBN : 958-33-7698-1
23. Franco, S.Guías de manejo de las valvulopatias aorticas. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2005. Manual condensado. Pgnas 177-182. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2005. 388 paginas. ISBN : 958-33-7698-1
24. Franco, S.Guías de manejo de las valvulopatias mitrales. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2005. Manual condensado. Pgnas 183-188. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2005. 388 paginas. ISBN : 958-33-7698-1
25. Jaramillo, J.S., Franco, S.Implante Quirúrgico del Electrodo Epicárdico en el Ventrículo Izquierdo Mediante Cirugía. En: Duque, M., Franco, S. Editores. Tratamiento no Farmacológico de la Falla Cardiaca. Sociedad Colombiana de Cardiología y Cirugía Cardiovascular. Primera Edición, Editorial Colina, Pgnas 89-92, Abril 2006. ISBN : 958-33-8661-8
26. Franco, S.Cirugía de Remodelación Ventricular en Falla Cardiaca. En: Duque, M., Franco, S. Editores. Tratamiento no Farmacológico de la Falla Cardiaca. Sociedad Colombiana de Cardiología y Cirugía Cardiovascular. Primera Edición, Editorial Colina, Pgnas 168 – 182, Abril 2006. ISBN : 958-33-8661-8
27. Jaramillo, JS., Franco, S., Vélez, JF. Revascularización Coronaria Quirúrgica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 559-576. ISBN : 958-33-9493-9
28. Franco, S., Vélez, JF, Jaramillo, JS., Cirugía en Enfermedad Valvular Aortica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 588 – 595. ISBN : 958-33-9493-9
29. Franco, S., Vélez, JF, Jaramillo, JS., Valvulopatia Mitral. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 596 – 603. ISBN : 958-33-9493-9
30. Franco, S., Vélez, JF, Jaramillo, JS., Cirugía en Enfermedad Valvular Pulmonar y Tricúspidea. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 604 – 606. ISBN : 958-33-9493-9
31. Jaramillo, JS., Franco, S., Vélez, JF, Disección Aortica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 607 – 617. ISBN : 958-33-9493-9
32. Franco, S., Vélez, A., Trauma de Corazón y Grandes Vasos. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 618 – 625. ISBN : 958-33-9493-9
33. Franco, S., Jaramillo, JS., Vélez, JF., Tumores Cardiacos. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 626 – 635. ISBN : 958-33-9493-9
34. Vélez, JF, Franco, S., Jaramillo, JS., Cardiopatías Congénitas del Adulto. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 649 – 659. ISBN : 958-33-9493-9
35. Uribe, W., Franco, S., Gil, E. Fibrilacion Auricular. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 441 – 466. ISBN : 958-33-9493-9
36. Restrepo, G., Franco, S.Endocarditis Infecciosa. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo VI, pgnas 614-30. ISBN : 958-97065-7-6
37. Franco, S., Sandoval, N. Tratamiento Quirurgico de la Fibrilacion Atrial. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo IX, pgnas 835-842. ISBN : 958-97065-7-6
38. Franco, S., Jaramillo JS. Trauma Cardiaco. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo XVI, pgnas 1442-49. ISBN : 958-97065-7-6
39. Franco, S., Velez, A. Trauma Vascular Cervical. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 31, P 425 – 433. ISBN : 979-958-98111-9-1
40. Franco, S., Velez, A., Jaramillo JS. Trauma Cardiaco. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 30, P 419 – 423. ISBN : 979-958-98111-9-1
41. Franco, S.Guias de Manejo de las Valvulopatias Aorticas. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 25, P 379 – 385. ISBN 978-958-98111-9-1
42. Franco, S.Guias de Manejo de las Valvulopatias Mitrales. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 26, P 387 – 392. ISBN : 979-958-98111-9-1
43. Jaramillo, J.S., Franco, S.Guias de Manejo de la Revascularizacion Coronaria Quirurgica. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin. Capitulo 24, P 369 – 377. ISBN : 979-958-98111-9-1
44. Franco, S.; Velez, JF.; Jaramillo,JS. Complicaciones mecanicas del infarto agudo del miocardio. En : Topicos Selectos en Enfermedad Coronaria – 2008. Velasquez, D. ed; Distribuna Ed, Cardiologia Clinica Medellin, 2008. P. 115-126. ISBN 978-958-8379-09-8
45. Jaramillo,JS.; Franco, S.; Velez, JF. Guias de manejo de la revascularizacion coronaria quirurgica. En : Topicos Selectos en Enfermedad Coronaria – 2008. Velasquez, D. ed; Distribuna Ed, Cardiologia Clinica Medellin, 2008. P. 197- 218. ISBN 978-958-8379-09-8
46. Franco, S.; Jaramillo, J.S. Guías de Manejo de la revascularización Coronaria Quirúrgica. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 429-440. ISBN : 978-958-8379-19-7
47. Franco, S.; Jaramillo, J.S. Guias de Manejo de las valvulopatias aorticas. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 441-448. ISBN : 978-958-8379-19-7
48. Franco, S.; Jaramillo, J.S. Guias de Manejo de las valvulopatias mitrales. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 449-456. ISBN : 978-958-8379-19-7
49. Franco, S.; Jaramillo, J.S. Trauma Cardiaco. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edición 2009, 503 paginas. P. 487-492. ISBN : 978-958-8379-19-7
50. Franco, S.; Jaramillo, J.S. Trauma Vascular Cervical. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edición 2009, 503 paginas. P. 493 – 503. ISBN : 978-958-8379-19-7
51. Franco, S.; Jaramillo, J.S. Trauma Vascular Cervical. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 501 – 511. ISBN : 978-958-8379-29-6
52. Franco, S.; Jaramillo, J.S. Trauma Cardiaco. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edicion 2010, 511 paginas. P. 495 – 500. ISBN : 978-958-8379-29-6
53. Franco, S.; Jaramillo, J.S. Guías de Manejo de las Valvulopatias Mitrales. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 457 – 463. ISBN : 978-958-8379-29-6
54. Franco, S.; Jaramillo, J.S. Guías de Manejo de las Valvulopatias Aorticas. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 449 – 456. ISBN : 978-958-8379-29-6
55. Franco, S.; Jaramillo, J.S. Guías de Manejo de la Revascularización Coronaria Quirúrgica. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 437 – 447. ISBN : 978-958-8379-29-6
56. Franco, S.; Bucheli, V. Anatomía Quirúrgica de la Válvula Mitral. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 26 – 31. ISBN : 978-958-44-7706-4
57. Franco, S.; Bucheli, V. Anatomía Quirúrgica de la Válvula Aortica. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 33 – 38. ISBN : 978-958-44-7706-4
58. Franco, S. Endocarditis Infecciosa. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 85 – 113. ISBN : 978-958-44-7706-4
59. Franco, S. Criterios para la Selección de una Prótesis Cardiaca. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 433 – 440. ISBN : 978-958-44-7706-4
60. Franco, S., Atehortua, M. Endocarditis Infecciosa. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 153 – 184. ISBN : 978-958-8379-46-3
61. Franco, S., Atehortua, M. Valvulopatia Mitral. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 717 – 727. ISBN : 978-958-8379-46-3
62. Franco, S., Atehortua, M. Cirugía Valvular Aortica. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 707 – 717. ISBN : 978-958-8379-46-3
63. Atehortua, M., Franco, S. Revascularización Coronaria Quirúrgica. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 675 – 690. ISBN : 978-958-8379-46-3
64. Atehortua, M., Franco, S. Evaluación y Momento Optimo de Intervención en el Paciente con Enfermedad Valvular Cardiaca. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 691 – 707. ISBN : 978-958-8379-46-3
65. Atehortua, M., Franco, S. Cirugía en Enfermedad Valvular y Tricuspidea. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 727 – 744. ISBN : 978-958-8379-46-3
66. Atehortua, M., Franco, S., Velez, L.A. Guias de Manejo de Revascularizacion Coronaria. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 619 – 630. ISBN : 978-958-8379-60-9
67. Velez, L.A., Franco, S., Atehortua, M. Guias de Manejo de las Valvulopatias Aorticas. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 631 – 642. ISBN : 978-958-8379-60-9
68. Atehortua, M., Franco, S., Velez, L.A. Guias de Manejo de las Valvulopatias Mitrales. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 643 – 653. ISBN : 978-958-8379-60-9
69. Velez, L.A., Atehortua, M., Franco, S. Cirugia en Enfermedad Valvular Pulmonar y Tricuspidea. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 655 – 661. ISBN : 978-958-8379-60-9
70. Franco, S., Bucheli, V., Atehortua, M., Velez, L.A. Guias de Manejo en Endocarditis Infecciosa En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 671 – 690. ISBN : 978-958-8379-60-9
71. Franco, S., Bucheli, V., Atehortua, M., Velez, L.A. Guias de Manejo de los Sindromes Aorticos Agudos. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 691 – 702. ISBN : 978-958-8379-60-9
72. Franco, S., Atehortua, M., Velez, L.A. Trauma Cardiaco. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 703 – 708. ISBN : 978-958-8379-60-9
Journal articles
1. Franco Sergio, Hincapié Miriam, Mejía Olga. Estudio Epidemiológico de Teníasis. Cisticercosis, San Vicente Antioquia – Colombia, 1985-1986. En: Medicina Tropical y Parasitología Vol. 2 No 1, Ecuador, Diciembre 1985.
2. Franco Sergio, Hincapié Miriam, Mejía Olga. Estudio Epidemiológico de Epilepsia y Neurocisticercosis. En: “Revista Universidad Industrial de Santander – Medicina¨ Vol. 14 No 1, Mayo 1986, p 143- 74.
3. Botero D., Franco S., Hincapié M., Mejía O. Investigaciones Colombianas Sobre Cisticercosis. En: Acta Neurológica. Vol. 2 No 2 Septiembre 1986, p. 3-6.
4. Franco Sergio; Londoño Juan. Dermatopoliomiositis – Reporte de un caso – Revisión del Tema. En: Medicina – U.P.B. Vol. 7 No 2, Noviembre 1988. p. 115.
5. Franco Sergio; Vásquez Jesús; Ortiz Jorge. Infarto Segmentario Idiopático del Epiplón Mayor – Presentación de dos casos y revisión del tema. En: Medicina – U.P.B. Vol. 10 No 2. Octubre. 1991, p. 109.
6. Franco Sergio. Choque Hipovolémico. Medicina U.P.B., Vol. 13 No 2, Octubre, 1994. P. 139-160.
7. Montoya A., Franco S.,. Lung Transplantation for Bronchoalveolar Cell Carcinoma. First Case Report in the Word Literature. 1996 – Loyola University Chicago Annual Report Magazine.
8. Franco S. Autopsy Results in Patients Following Lung Transplantation. Department of Pathology at Loyola University Medical Center. 1996 – Loyola University Chicago Annual Report Magazine.
9. Franco S., Giraldo N., Flórez M. Tratamiento Quirúrgico de la Coartación Aórtica Seguimiento a Largo Plazo – 8 años. Revista Colombiana de Cardiología. Vol. 5 No 5, Diciembre 1996.
10. Franco S, Giraldo N. Trauma Cardíaco: Revisión del Tema. Revista Colombiana de Cardiología. Marzo de 1997.
11. Franco S., Giraldo N., Ramírez C., Vallejo C., Castro H. Revascularización Miocárdica en pacientes con fracción de eyección menor del 30%. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 301.
12. Franco S., Giraldo N., Fernández H., Ramírez C., Vallejo C., Castro H. Transección Aórtica Traumática: Presentación de tres casos, revisión de la literatura. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 330.
13. Franco S., Giraldo N., Vélez S. et al. Fístula de la arteria coronaria derecha al tracto de salida del ventrículo derecho. Reporte de un caso – revisión del tema. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 319.
14. Giraldo N., Franco S., Ramírez C., Vallejo C., Castro H. CIV y Banding de la arteria pulmonar en un paciente adulto. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 333.
15. Giraldo N., Franco S., Ramírez C., Vallejo C., Castro H. Ruptura Ventricular post implantación de válvula mitral. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 340.
16. Castro H., Ramírez C., Franco S., Mesa J. et al. Anestesia y técnica quirúrgica en pacientes sometidos a implantación percutánea de endoprótesis en aneurismas de la aorta abdominal. Reporte de tres casos y revisión de la literatura. Departamento de Cirugía y Anestesia Cardiovascular. Departamento de Hemodinámica. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 331.
17. Vallejo C., Castro H., Ramírez C., Franco S., Duque M. et al. Anestesia y técnica quirúrgica en pacientes sometidos a implante de cardiodesfibrilador automático. Reporte de 20 casos. Departamento de Cirugía y Anestesia Cardiovascular. Departamento de Electrofisiología y Arritmias. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
18. Ramírez C., Vallejo C., Castro H., Franco S., Giraldo N. et al. Protección Miocárdica: Solución de HTK en Cirugía Cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
19. Ramírez C., Vallejo C., Castro H., Franco S., Giraldo N. et al. Protección Miocárdica: Comparación entre la Solución de HTK y la Solución de Buckberg en Cirugía Cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
20. Vallejo C., Ramírez C., Castro H., Giraldo N., Franco S. Hipotiroidismo y enfermedad cardiaca: Administración de hormona tiroidea vía oral en pacientes sometidos a cirugía cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 334.
21. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Revascularización miocárdica con arteria radial: Estudio de Casos y Controles. Departamento de Cirugía Cardiotorácica, Clínica Medellín. XIX Congreso Colombiano de Cardiología. Noviembre 27 – Diciembre 1, 2001. Revista Colombiana de Cardiología, 2001, Vol. 9(2): 197.
22. Giraldo, N., Franco, S., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Revascularización miocárdica Off Pump: Requerimiento de derivados sanguíneos. Departamento de Cirugía Cardiotorácica, Clínica Medellín. XIX Congreso Colombiano de Cardiología. Noviembre 27 – Diciembre 1, 2001. Revista Colombiana de Cardiología, 2001, Vol. 9(2): 238.
23. Giraldo, N., Franco, S. Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Endarterectomia Coronaria del tronco principal izquierdo. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES Medicina Vol. 16 # 1, página 39-44. Enero-Marzo 2002.
24. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Cierre tardío del esternón en el manejo del sangrado mediastinal post cirugía cardiaca. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES – Medicina. Vol. 16 # 1, página 27-34. Enero-Marzo 2002.
25. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Cambio valvular mitral con preservación total del aparato valvular: Técnica quirúrgica, resultados y seguimiento. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES Medicina. Volumen 16 # 1, página 9-18. Enero-Marzo 2002.
26. Franco S, Giraldo N, Escobar A, Fernández H, Vallejo C, Ramírez C. Cambio valvular mitral con preservación total del aparato valvular: técnica quirúrgica, resultados y seguimiento. Revista Colombiana De Cardiología. 2003. pp. 368 – 74
27. Giraldo N, Franco S, Escobar A, Fernández H, Vallejo C, Ramírez C. Cierre tardío del esternón en el manejo del sangrado mediastinal post cirugía cardiaca. Revista Colombiana De Cardiología 2003. pp. 95 – 99
28. Escobar A., Giraldo N., Franco S., Jaramillo J., Orozco A. Taquiarritmias supraventriculares postcirugia cardiaca con y sin el uso de circulación extracorpórea. En : CES Medicina Volumen 17 # 1, Enero-julio 2003, Pgnas 23-31
29. Echeverri JL, Gonzáles M, Franco S., Vélez LA. Ruptura traumática de la aorta. Reporte de dos casos y revisión de la literatura. Medicina Crítica y Cuidados Intensivos. Enero – Junio 2004, 2 (1) : 31-35
30. Franco, S. Giraldo, N., Gaviria, A. et al. Aneurismas y seudoaneurismas de injertos venosos coronarios. Revista Colombiana de cardiología, Vol. 11 # 8, Abril 2005. Pgna 401- 404.
31. Franco, S.; Uribe, W.; Velez, JF. et al. Tratamiento quirurgico curativo de la fibrilacion atrial mediante tecnica de ablacion con radiofrecuencia monopolar irrigada : resultados a corto y mediano plazo. Revista Colombiana de Cardiologia. 2007. Vol 14, # 1. Pnas 43 – 55.
32. Escobar, A., Franco,S., Giraldo,N., et al. Tecnica de perfusion selectiva cerebral via subclavia para la correccion de patologias del arco aortico. Revista Colombiana de Cardiologia Volumen 14, numero 4, agosto 2007. P 232-237
33. Franco, S.Tratamiento quirurgico de la fibrilacion atrial. Revista Colombiana de Cardiologia – Guias de Diagnostico y Tratamiento de la Fibrilacion Auricular. Vol 14, Suplemento 3, Octubre 2007. P. 133 – 143.
34. Franco, S. Velez, A., Uribe, W., Duque, M., Velez, JF, et al. Tratamiento quirurgico de la fibrilacion atrial mediante radiofrecuencia. Revista Medica Sanitas 2008, Volumen 11, Numero 1, pgnas 8 – 20. Febrero – Abril, 2008.
35. Franco,S., Herrera, AM., Atehortua, M. et al. Use of Steel bands in sternotomy closure : implications in high-risk cardiac surgical population. Interactive CardioVascular and Thoracic Surgery 8 (2009) : 200-205.
36. Franco, S.Tratamiento Quirurgico para el manejo de las arritmias ventriculares. Guias Colombianas de Cardiologia. Artitmias Ventriculares y Muerte Subita. Revista Colombiana de Cardiologia. Volumen 18, Suplemento 1. Pgnas 160 – 163. Febrero 2011.
37. Miranda, A. ; Franco, S.,; Uribe, W. et al. Tromboembolismo Pulmonar Masivo de Alto Riesgo. Medicina ( Buenos Aires), 72 : 2012; Pgnas 128-130.
38. Miranda, A., Duque, M., Franco, S., Velasquez, J. et al. Tromboembolismo Pulmonar Masivo. Indicaciones de Cirugia – Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1. Marzo de 2012.
39. Franco, S.; Eusse, A.; Atehortua, M., Vélez, L., et al. Endocarditis Infecciosa : Análisis de Resultados del Manejo Quirúrgico Temprano. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 66. Marzo de 2012.
40. Franco, S.; Bucheli, V.; Atehortua, M., Vélez, L.; Eusse, A et al. Tratamiento Quirurgico : El “Gold Estándar” en el manejo de los defectos del septum interauricular. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1. Marzo de 2012.
41. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., et al. Anomalías coronarias del Adulto. Origen anómalo de la arteria coronaria izquierda de la arteria pulmonar (ALCAPA). Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 61. Marzo de 2012.
42. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., et al. Metástasis cardiaca de carcinoma anaplasico de tiroides. Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 70. Marzo de 2012.
43. Franco, S.; Giraldo, N.; Atehortua, M., Vélez, L.; Castro, H., et al. Endarterectomia coronaria del tronco principal izquierdo : Seguimiento a 15 años. Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 66. Marzo de 2012.
44. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., Bucheli, V.; et al. Implante de válvulas biológicas : evaluación de libertad de reoperación por deterioro valvular estructural. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 69. Marzo de 2012.
45. Miranda, A. Franco, S. Uribe, W., Duque, M. et al. Tromboembolismo Pulmonar Masivo de Alto Riesgo Asociado a Foramen Ovale Permeable. Medicina (Buenos Aires) 72 : 128 – 130. 2012.
46. Franco, S.Criterios Para la Selección de Una Protesis Cardiaca. Rev Fed Arg Cardiol. 2012; 41(3): 156 – 160.
Special topics in Cardiac Surgery: (Monographs)
1. Franco Sergio. Manejo Básico Inicial del Paciente Con Trauma CortoPunzante En: Monografía. Hospital San Vicente de Paúl – Prado (Tolima) 1989.
2. Franco S; Montoya A. Transplante Pulmonar: Indicaciones, Criterios de Selección y rechazo, Técnica Quirúrgica, Manejo de Donante y receptor, Complicaciones. Protocolo para la realización de transplante pulmonar en nuestro medio. Comité de transplantes de corazón y pulmón. 1996. Clínica Cardiovascular Santa María, Biblioteca Médica – Facultad de Medicina, Universidad Pontificia Bolivariana
3. Giraldo N., Franco S., Estudiantes X Semestre Instituto de Ciencias de la Salud – CES. Tratamiento Quirúrgico de la Endocarditis Infecciosa. Monografía. Investigación realizada en la Clínica Cardiovascular Santa Maria. Publicación Monográfica. Enero 1997.
4. Franco S. Safenectomía Videoendoscópica. Realización de video con descripción de la técnica quirúrgica. Descripción Monográfica. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. Diciembre de 1997.
5. Franco S., Giraldo N., Fernández H. Tratamiento Quirúrgico de la Enfermedad Pulmonar Obstructiva Crónica. Cirugía de Reducción de Volumen Pulmonar. Monografía, Departamento de Cirugía Cardiovascular – Unidad Cardiovascular Clínica Medellín. Octubre 1999.
6. Franco S., Escobar A. Trauma de Tórax. Revisión del tema. Monografía. Departamento de Cirugía Cardiovascular / Unidad Cardiovascular Clínica Medellín. Octubre de 1999.
7. Franco S., Jaramillo J.C. Cirugía en el paciente con Angina. Consenso Nacional sobre el Manejo de la Angina de Pecho. Sociedad Colombiana de Cardiología. Bogota, 11-12 agosto 2000.
8. Franco, S. Fibrilación Atrial: Tratamiento Quirúrgico. I Actualización del Consenso Nacional Sobre Fibrilación Atrial. Capitulo de Electrofisiología, Sociedad Colombiana De Cardiología. Abril 2002.
9. Franco, S, Jaramillo JS, Vélez JF, Castro H. Infecciones Mediastinales. Monografía. Departamento de Cirugía Cardiovascular. Hospital Departamental Santa Sofía de Caldas, Manizales. Mayo de 2003.
10. Guias Colombianas de Cardiologia. Fibrilacion Atrial – Guias de bolsillo.
Duque, M, Marin, J, ed. Franco, S. Cirugia de fibrilacion atrial. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. 2008.
11. Franco, S. Long-Term Effectiveness of HIFU on Atrial Fibrillation in High Risk Valvular Surgery Patients. A Clinical Interview from Epicor- Cardiac Ablation System – St Jude Medical. March 2009.
I apologize for the wordiness of this post – but much of what we discuss below is covered in the Bogotá, Cartagena and Mexicali books – the essential mechanisms of cardiac surgery; how procedures work, what is off-pump surgery, when do we use the bypass pump and other explanatory information. But since I have am not writing a full book on Medellin, I wanted to offer a bit of a primer for my new internet readers here.
Dr. Luis Meza
Cardiac surgeon, Hospital General de Medellin
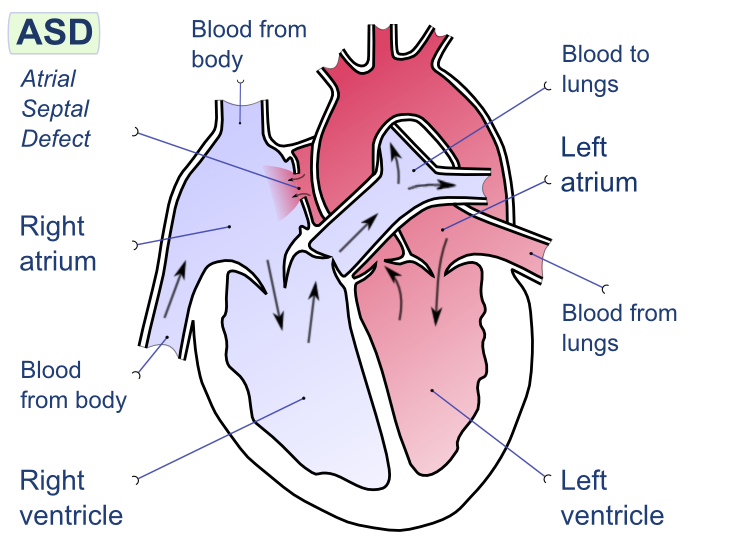
After interviewing Dr. Meza and meeting many of the staff at Hospital General de Medellin, it was a pleasure to be invited to observe Dr. Meza and Dr. Urequi , the head of the cardiac surgery department in the operating room. Despite the patient’s young age, the surgery (for me as an observer) was knuckle-biting. While the surgery itself was a fast, straight-forward and uncomplicated repair of an interauricular septal defect – it was the patient’s fragile condition that had me on the edge of my seat.
Complex patients The case was typical of many of the cases they see at public hospitals. It was a young patient with newly diagnosed right-sided heart failure due to an uncorrected congenital defect. The patient had traveled from another part of Colombia (one of the poorer regions) to have surgery. The patient had initially presented to a local doctor after a syncopal event (passing out) and was found to have an enlarged heart, with a moderate sized pericardial effusion (fluid in the sac around the heart.) After arriving at HGM, the patient was also diagnosed with a serious acquired coagulopathy (bleeding disorder).
drawing courtesy of Wikipedia (Creative Commons licensing)
Since the patient had a hole between the left atrium leading into the right atrium, blood was being pushed from the left atrium (which is under higher pressure) to the low pressure right atrium. Over the course of many years, this had caused the right atrium to enlarge massively. As the right atrium was continuously being overfilled (from blood from the left side), the right side of the heart was being forced to work harder, and harder. As the atrium continued to be overstretched, and enlarged – it also caused blood to be forced back into the pulmonary arteries – causing pulmonary hypertension. While pre-surgical tests (echocardiogram, and cardiac catheterization) showed the patient to have (only) moderate pulmonary hypertension (with PA systolic pressures of 65mmHg).
Pre-operative testing is only part of the story
However, when we looked down, into the patient’s chest – it was obvious that the patient’s pulmonary vasculature was engorged and enlarged. The patient’s heart was massive, and floppy (which is a sign the heart is working way too hard). The patient also had peripheral edema which is another sign that the heart was not working well.
Potential for badness*
So even though, the surgery itself (described below) is not terribly technically challenging (‘like darning socks’ one surgeon used to say) – a lot can go wrong because the patient’s heart just doesn’t work that well to begin with.
* a not-so-scientific term to describe the likelihood of potential complications, problems or adverse outcomes. These may be unavoidable circumstances in many cases – but the term is a reminder to remain vigilant even during so-called “simple” procedures.
Nitric oxide on hand
This OR does have nitric oxide – (which we didn’t need), but was available nearby, just in case. Nitric oxide, milrinone and other medications are critical to have on hand in patients with pulmonary hypertension. Some patients will never need it – others can’t survive without it – and sadly, (in patients with severe fixed pulmonary hypertension), nothing – not even an assist device is going to make much difference. While we can try to predict which patients are going to tolerate surgery, it’s not always clear-cut. Tests (echocardiograms, right heart caths) can predict, tests can give probabilities – but sometimes tests are wrong, and patients who appear to have only ‘mild’ disease do very poorly (and visa versa). Sometimes, we just have to hold our breath as the patient comes off bypass and see.
canisters of nitric oxide in OR #1
As I mentioned in a previous post – cardiac surgery procedures can be a bit more complicated than many other surgical procedures, and while having something like nitric oxide on hand doesn’t seem like a big deal – it is. (I have worked in several facilities without these capabilities). It also speaks to the general preparedness of the staff. But despite the ‘potential for badness’ everything proceeded beautifully with Drs. Urequi and Meza. The case seemed to speed by despite the patient’s fragile health. The entire CPB (cardiopulmonary bypass run) was just 26 minutes with a total cross-clamp time of 31 minutes.)
A little bit about cardiopulmonary bypass – the “heart-lung machine”
In comparison to the congenital repair above, average CPB times for valve replacement run around 100 minutes, 60 to 90 minutes for bypass surgery. Patients have a higher risk of CPB related complications from hypo/ altered perfusion after long pump runs . As the clock begins to exceed 120 minutes, the risk of renal failure, cognitive changes and bleeding problems (as blood cells are continuous smashed/ broken / damaged within the pump) increase.
What is “Off-pump surgery”? Nowadays, lots of people get real excited about “off-pump” surgery because they think that by not using the heart-lung machine, they can avoid a lot of the problems we mentioned above. But that’s oversimplifying the entire scenario – and one that I find is often used to “sell” a particular surgeon or surgical program. Off-pump can be safer than CPB cases, for some patients. But these are usually not the patients that the surgery is sold to.. So it’s important to know what some of the terminology really means. Just because Hospital X has billboards announcing that they now perform off pump surgery – doesn’t mean that it’s something you may even need or want.
Off pump is not for everyone
Patients have to be fairly healthy to tolerate cardiac surgery without the pump. People with a lot of the problems that we thought were worsened by the pump, actually fare worse when we try to do surgery without the heart-lung machine. For example, we initially thought that Off-pump surgery would be great for people with renal insufficiency or ‘bad kidneys’ – particularly people who have kidney problems but aren’t quite sick enough to be on dialysis yet. The hope was that by avoiding the bypass pump we could avoid any damage to the kidneys from artificial flow/hypoperfusion because one of the biggest risks of cardiac surgery in patients with bad kidneys is that surgery will cause their kidneys to fail entirely, and make patients dialysis dependent. Unfortunately, the research from all of the off-pump surgeries being done hasn’t really shown the benefits that we thought it would. So like most things in medicine, it’s not quite the panacea we had hoped it was. But we did learn an incredible amount of information once surgeons started trying off pump surgeries for coronary bypass. Surprisingly, we learned that many of the complications, and conditions that we had long blamed on the CPB pump – weren’t related to the machine at all. But much of this is still being argued by cardiac surgeons every single day – each with different research studies giving different results..
More importantly, Off-pump not possible for many types of cardiac surgery
It’s technically impossible to do some types of cases without the bypass pump. Coronary bypass surgery (CABG) is very different from other types of surgery, for example. During bypass, the surgeon is only operating on the outside of the heart – attaching new conduit (arteries and veins) to arteries on the surface of the heart. So – it isn’t absolutely essential to have the pump circulating blood for him while he’s operating – in some patients – we can let their body do it for us during surgery.
But replacing diseased heart valves, or the great vessels (aortic aneurysms etc) is a completely different entity. In those surgeries – the surgeon is cutting into the heart or great vessels themselves. It’s not possible to lop off the top of the aorta, operate on the aortic valve and not have blood being re-directed mechanically during this process. Otherwise blood would just literally spill out into the chest and never oxygenate the brain and the rest of the body. (The only time we ever do this kind of procedure without a pump is during organ retrieval – for obvious reasons). It’s important to know these distinctions so people understand how the surgery actually proceeds.
For the case today – the surgeon has to make an incision through the side of the atria (wall of the heart chamber) to get to the hole on the inside wall of the heart.) The surgeon then closes the hole with suture (and a patch, in some cases). Some doctors do this in the cath lab without surgery – but that’s also controversal because the patch used in the cath procedures in the past has caused a high incidence of stroke. In a young patient like the one here – you certainly wouldn’t want to risk it – particularly since we don’t know how well those patches hold up in the long term.
Cardiac surgeons operate at Hospital General de Medellin (HGM)
Overall evaluation of today’s case:
Safety checklists, and all pre-operative procedures were completed. Patient was prepped and draped in an appropriate sterile fashion. Antibiotics were administered within the recommended window (of time). Appropriate records were maintained during the case.
Surgery proceeded normally and without incident.
Due to an underlying coagulopathy the patient did require administration of nonautologous blood products (4 units of packed red blood cells, 3 packets of platelets, and abumin) while on pump. While the facility does not have a ‘cell-saver’ for washing and re-infusing shed blood, patient did receive autologous(their own) transfusion from the CPB pump. This blood, from the CPB circuit was returned to the patient to limit the amount of blood needed after surgery. Hemoglobin at the conclusion of surgery was 9.6mg/dl, which is within acceptable parameters.
Hemostasis was obtained prior to chest closure, with only a small amount of chest tube drainage in the collection chamber at the time of transfer to the intensive care unit.
Surgical Apgars – do not apply for cardiac cases due to the nature of the case, and use of CPB. Mean pressure while on CPB was within an acceptable range. Patient’s urinary output was less than anticipated during the case (150cc) despite the use of mannitol while on pump, but the patient responded well (1000+) with volume infusion and the addition of furosemide.
The patient was hemodynamically stable during the entire case. The was a very brief transitory period of hypotension (less than 5 minutes) near the conclusion of the case, which was immediately noted by anesthesia and treated with no recurrence.
On transfer to the unit, the patient was accompanied by several members of the OR staff, including Dr. Meza, the anesthesiologist, and the perfusionist, each of which did a face-to-face “hand-off” report of the patient (and medical history) including the course of the surgical procedure (including medications given, lab values, procedural details) to the Intensivist (physician), with ICU nursing staff attending to the patient.
Transesophageal echo (TEE) was not performed during this case, but was available if needed.
Also, I am happy to report there were no smartphones or “facebooking” in sight. No one appeared engaged in anything other than the surgery at hand.
If you’ve never been to the cardiac operating room – it’s a completely different world, and not what most people expect. For starters, unlike many areas of health care (particularly in the USA), the cardiac operating room is usually very well staffed.
Just a few of the people working in the OR. (photo edited to preserve patient privacy)
For example, there were eight people working in the operating room today:
Dr. Suarez observes her patient during surgery. (photo edited to preserve patient’s privacy)
Ms. Catherine Cardona, “Jefe”/ Nurse who supervises the operating room
Ms. Diana Isobel Lopez, Perfusionist (In Colombia, all perfusionists have an undergraduate degree in nursing, before obtaining a postgraduate degree in Perfusion). The perfusionist is the person who ‘runs’ the cardiac bypass machine.
Ms. Laura Garcia, Instrumentadora (First Assist)
Angel, circulating nurse
Olga, another instrumentadora, who is training to work in the cardiac OR.
This is fairly typical for most institutions.
Secondly – it’s always a regimented, and checklist kind of place. (I wish I could say that about every operating room – but it just wouldn’t be true.) But cardiac ORs (without exception) always follow a very strict set of accounting procedures..
For starters – there are labels.. For the patient (arm bands), for the equipment (medications, blood products etc..) even the room is labeled.
Sign on operating room door (edited for patient privacy)
Then come the checklists..
Perfusionist Diana Lopez gathers information to begin her pre-operative checklist.
The general (WHO) operating room checklist. The perfusionist’s checklist.. The anesthesiologist’s checklist.. and the big white cardiac checklist.
by the end of the case, this board will be full..
The staff attempts to anticipate every possible need and have it on hand ahead of time. Whether it’s nitric oxide, blood, defibrillation equipment, or special medications – it’s already stocked and ready before the patient is ever wheeled in.
Most of these things are universal:
such as the principles of asepsis (preventing infection), patient safety and preventing intra-operative errors – no matter what hospital or country you are visiting (and when it comes to surgery – that’s the way it should be.)
Today was no exception..
In health care, we talk about “OR people” and “ER people”.. ER people are the MacGyvers of the world – people who thrive on adrenaline, excitement and the unexpected. They are at their best when a tractor-trailer skids into a gas station, ignites and sets of a five-alarm fire that decimates a kindergarden, sending screaming children racing into the streets.. And God love them for having that talent..
But the OR.. that’s my personal area of tranquility.
This orderly, prepared environments is one of the reasons I love what I do.. (I am not a screaming, “by the seat-of-your-pants”/ ‘skin of your teeth’ kind of gal). I don’t want to encounter surprises when it comes to my patient’s health – and I never ever want to be caught unprepared. That’s not to say that I can’t handle an emergent cardiac patient crashing in the cath lab – it just means I’ve considered the scenarios before, (and have a couple of tricks up my sleeve) to make sure my patient is well taken care of (and expedite the process).
That logical, critical-thinking component of my personality is one of the reasons I am able to provide valuable and objective information when visiting hospitals and surgeons like Dr. Urequi’s and Dr. Meza’s operating room at Hospital General de Medellin.
In OR #1 – cardiothoracic suite
As I mentioned in a previous post on Hospital General de Medellin, operating room suite #1 has been designated for cardiac and thoracic surgeries. This works out well since the operating room itself, is modern and spacious (which is important because of the area needed when adding specialized cardiac surgery equipment like the CPB pump (aka heart-lung machine). There are muliple monitors, which is important for the video-assisted thoracoscopy (VATS) thoracic cases but also helpful for the cardiac cases. The surgeon is able to project the case as he’s performing it on a spare monitor, which allows everyone involved to see what’s going on during the case (and anticipate what he will need next) without shouting or crowding the operating room table.
Coordinating care by watching surgery
For instance, if the circulator looks up at the monitor and sees he is finishing (the bypasses for example), she can make sure both the instrumentadora and the anesthesiologist have the paddles and cables ready to gently defibrillate the heart if it needs a little ‘jump start’ back into normal rhythm..or collect lab samples, or double check medications, blood products or whatever else is needed at specific points during the surgery.
Dr. Luis Fernando Meza Valencia, cardiac surgeon and his wife, Dra. Elaine Suarez Gomez, anesthesiologist have a terrific partnership as part of the Cardiac Surgery program at Hospital General de Medellin (HGM). (Hospital General de Medellin is one of just a few public hospitals that have heart surgery programs.)
Dr. Meza, a Cali native who trained at Fundacion Cardioinfantil under the instruction of Dr. Pablo Umana, Dr. Nestor Sandoval along with Dr. Maldonado now performs coronary bypass, valve replacement, surgery on the great vessels (such as ascending arch replacement, aortic aneurysm repair) at the Hospital General de Medellin as well as several smaller, private facilities like Clinica Las Vegas.
He has worked at HGM for 2 1/2 years since he moved from the public hospital in Manizales (in the coffee-growing region of central Colombia).
Dra. Elaine Suarez is a anesthesiologist who has specializes in cardiothoracic anesthesia. She has been practicing for five years and is fluent in English and German in addition to her native Spanish.
High risk patients
Because HGM serves the public and many of their patients are impoverished, Dr. Meza and Dra. Suarez see a large number of rheumatic heart disease and endocarditis patients. Many of these patients have had very limited preventative care or medical management of their underlying chronic health conditions. A large number of these patients have significant co-morbid conditions such as diabetes, chroic pulmonary disease, hypertension, hyperlipidemia, and nephropathies (kidney damage). This subset of patients almost always presents in the midst of a cardiac emergency.
In the Consulta Externa
Dr. Meza reports that he usually spends at least an hour with his patients during the initial consultation, gathering information, examining the patient and explaining the necessary tests and treatments.
In the Operating Room
Haven’t had an opportunity to follow Dr. Meza to the operating room yet, but we did get to see Dra. Suarez in action.
Long time readers (and former patients) will be familiar with my aspirin mantra but now Medscape has published a CME course by Dr. Desiree Lie for health care providers in primary practice, general surgery (and other areas that may not be familiar with post-cardiac patient recommendations.) As I may have mentioned before, in cardiac surgery – we routinely start aspirin in our patients prior to bypass surgery.
Know the most current recommendations for aspirin and surgery
Don’t stop Aspirin before surgery
I’ve converted the CME course, Don’t stop Aspirin before surgery into a pdf – but if you want credit – you will have to go to Medscape and log in. (For everyone else – it’s a nice read – and explains the importance of continuing aspirin in patients who are taking it for “secondary prevention” or are at high risk of cardiovascular events.
That’s because the complications of discontinuing aspirin therapy in these patients are WORSE than the minor risk of bleeding. (Bleeding issues for most patients taking aspirin are fairly minor.. Now, clopidogrel (Plavix) and prasugrel (Effient) are another story!)
Wait a second… What’s secondary prevention?
They way to think about secondary prevention is “closing the barn after the cows are loose,” as one of my colleagues explains it. This means that Aspirin has been prescribed to these patients after something has already happened – like a stroke, a heart attack, stents or cardiac surgery. So in these patients – secondary prevention can be thought of as preventing a second event or further complications from a disease process we already know about.
Now, patients that are at high risk for cardiovascular events like diabetics or people with other kinds of blockages (peripheral vascular disease, renal artery stenosis) haven’t had a heart attack yet – but we think that they are at a high risk of this happening – so they take aspirin to prevent this (primary prevention).
In people who are at low or moderate risk – low cholesterol, nonobese, normal glucose, nonsmokers: these people may take aspirin, but (probably not prescribed) and it is safe for them to discontinue aspirin before surgery.
But in the first two classes of patients (secondary prevention group/ high risk group) – stopping aspirin may actually INCREASE the risk of having a heart attack, stroke or other thrombotic event during surgery. But if you are having surgery – be sure to check with your cardiologist or cardiac surgeon before. Don’t rely on your PCP or general surgeon (it’s not their area of expertise) and they may not be up-to-date on the latest recommendations [hence the continuing education course].
As always – these posts are not medical advice – but should serve as talking points for patients when soliciting medical advice from their healthcare providers.
It looks like the rest of the medical community is finally speaking up about the overuse and safety issues of TAVI/ TAVR for aortic stenosis, but it’s still few and far between – and in specialty journals… But in the same week that Medscape, and the Heart.org reported on a newly published article in the British Medical Journal on the overuse of TAVI therapies, and the need for earlier diagnosis and treatment of Aortic Stenosis – the Interventionalists over at the Heart.org (a cardiology specialty journal) have published a series of articles promoting / pushing the procedure including an article entitled, “The TAVR Heart team roles.”
JAMA recently published a paper by Robert Bonow and Chintan Desnai, discussing the benefits, risks and expectations with TAVI. This paper discusses the very real need for clinicians to address heightened patient expectations regarding TAVI as an ‘easy’ alternative to surgery.
Here at Cartagena Surgery – we’ve been doing our own research – contacting and talking to a multitude of practicing cardiologists and cardiac surgeons to get their opinions – in addition to reviewing the latest data.
In related news, a review of the latest research on the ‘transcatheter’ valve therapies demonstrates considerable concern: including data on peri-valvular leaks as reported in the last national TAVI registries in Europe and in the US:
• The incidence of paravalvular leaks after TAVI is extremely high ( > 60%)
• It is technically challenging today to quantify these leaks.
• Most of them are quoted “mild”, but more than 15 % are estimated “moderate” and “severe”.
• In > 5% of patients, the peri-valvular or valvular regurgitation grade increased significantly over time.
• there is no significant difference between Edwards SAPIEN and Medtronic COREVALVE
As one cardiologist explained:
“Importantly, the thrombogenic potential of mild leaks was recently demonstrated by Larry Scotten ( Vivitro System Inc. Victoria, Canada). High reverse flow velocities expose glycoprotein GP Ib-IX-V platelet receptors to circulating Von Willebrand molecule with, as results, platelet aggregation and fibrin formation. The incidence of brain spots and stroke after TAVI was of great concern in the PARTNER A and B studies. Whereas, Aspirin is not mandatory in patients implanted with bioprosthetic valves, Plavix + Aspirin is recommended for all TAVI patients. The rationales of such therapy were not explained so far.”
Valve oversizing – a surgeon explains
“To reduce these peri-valvular leaks , cardiologists tentatively use large valve size, up to 29-mm. The very large majority of valve sizes used in conventional aortic valve replacement are smaller than 25-mm. Oversizing may increase the risk of late aortic aneurysms (aortic rupture has been reported) [emphasis added].
Moreover, atrio-ventricular conduction may be impaired with the need of permanent pacing. Poorer outcomes have been reported in patients when the need for permanent pacemaker occurs.
“As we like to say about clothes and shoes, you forget the price overnight but you remember the quality for ever . The price of TAVI may be cheaper but patients may experience inferior outcomes. In view of these results, using TAVI would not be appropriate for the great majority of heart valve candidates. Moreover trans-catheter delivery and sub-optimal fit are not likely to increase tissue valve durability… and everybody knows that tissue valves are not enough durable for young adults and children. TAVI is thus a suitable strategy only for the neglected population of high risk patients who are no longer candidates for surgery [emphasis added].
Worth pointing out again that there would be no need for TAVI and long-term outcomes of patients would be much better if severe aortic stenosis were correctly managed at the right time. Enclosed the recommendations of Robert Bonow (Circulation, July 25, 2012) for early valve replacement in ASYMPTOMATIC patients. A large cohort of accurate biomarkers is available today for correct timing of surgery and consequent prevention of irreversible myocardium damage. In the study of Lancellotti (enclosed) 55% of “truly asymptomatic patients” with severe aortic stenosis developed pulmonary hypertension during exercise and had poor clinical outcomes. The measurement of both mean trans-aortic pressure gradient and systolic pulmonary pressure, which are technically easy, rapid and with good reproducibility may improve the management of such patients.
These updates on the natural history of aortic stenosis illustrate the present paradoxical and intriguing focus of the industry on an experimental procedural innovation for end-stage old patients when more efficient heart valves are today feasible and could be used sooner for the benefit of all patients .
Modified from Ross J and Branwald E (Circulation 1968 (Suppl): 61-67)
• The incidence of stroke was 9% after TAVI in the 214 patients of the enclosed study published last week in the American Journal of Cardiology. The incidence of stroke with TAVI was > two times higher than with conventional surgery in the PARTNER study. Pooled proportion of postoperative stroke was 2.4% with conventional surgery in the large meta-analysis of patients > 80 years old (enclosed)
• Peri-valvular aortic insufficiency is observed in more than 60% of patients undergoing trans-catheter aortic valve replacement. Moderate or severe aortic insufficiency was seen in 17.3 % of the PARTNER inoperable and high risk cohorts at 1 year. They have been reportedly associated with dyspnea, anemia, cardiac failure and diminished survival. Most interestingly, the FDA does not accept more than 1% peri-valvular insufficiency in patients implanted with conventional prosthetic heart valves… The SJM Silzone mechanical heart valve was re-called because of peri-valvular leakage rate of… 1.5 % .
• Traditionally, aortic stenosis involving a 2-cuspid aortic valve has been a contraindication to TAVI. Of 347 octogenarians and 17 nonagenarians explanted valves , 78 (22%) and 3 ( 18%) had stenotic congenitally bicuspid aortic valve, respectively. Because the results of TAVI are less favorable in patients with stenotic congenitally bicuspid valves, proper identification of the underlying aortic valve structure is critical when considering TAVI in older patients . More than 50% of patients with aortic stenosis have bicuspid aortic valve and are not, therefore, good candidates for TAVI. Most importantly, the great majority of patients with calcified stenotic bicuspid aortic valves is young ( < 60 years old) and not candidate for tissue valve replacement.
• The French Registry of trans-catheter aortic-valve implantation in high-risk patients was published in the New England Journal of Medicine on May 3, 2012. It reports 3195 TAVI procedures during the last two years at 34 centers.
The mean age was 83 years. The incidence of stroke was 4.1%. Peri-prosthetic aortic regurgitation was 64 %. The rate of death was 24% at one year. At the same time, the meta-analysis published in the American Heart Journal reports 13,216 CONVENTIONAL AORTIC VALVE REPLACEMENT in patients > 80 years old. The rate of death was 12.4% at one year, 21.3% at 3 years and 34.6% at 5 years
Full references for works cited in text:
Bonow, R. O. (2012). Exercise hemodynamics and risk assessment in asymptomatic aortic stenosis. Circulation 2012, July 25.
Lancelloti, P., Magne, J., Donal, E., O’Connor, K., Dulgheru, R., Rosca, M., & Pierard, L. (2012). Determinants and prognostic significance of exercise pulmonary hypertension in asymptomatic severe aortic stenosis. Circulation, 2012 July 25.
Takkenberg, J. J. M., Rayamannan, N. M., Rosenhek, R., Kumar, A. S., Carapitis, J. R., & Yacoub, M. H. (2008). The need for a global perspective on heart valve disease epidemiology: The SHVG working group on epidemiology of heart disease founding statement. J. Heart Valve Dis. 17 (1); 135 – 139.
Gilard M, Eltchaninoff H, Iung B, Donzeau-Gouge P, Chevreul K, Fajadet J, Leprince P, Leguerrier A, Lievre M, Prat A,Teiger E, Lefevre T, Himbert D, Tchetche D, Carrié D, Albat B, Cribier A, Rioufol G, Sudre A, Blanchard D, Collet F, Dos Santos P, Meneveau N, Tirouvanziam A, Caussin C, Guyon P, Boschat J, Le Breton H, Collart F, Houel R, Delpine S,Souteyrand G, Favereau X, Ohlmann P, Doisy V, Grollier G, Gommeaux A, Claudel JP, Bourlon F, Bertrand B, Van Belle E, Laskar M; FRANCE 2 Investigators. Collaborators (184). Registry of transcatheter aortic-valve implantation in high-risk patients. N Engl J Med. 2012 May 3; 366(18):1705-15 [full abstract below].
BACKGROUND:
Transcatheter aortic-valve implantation (TAVI) is an emerging intervention for the treatment of high-risk patients with severe aortic stenosis and coexisting illnesses.
We report the results of a prospective multicenter study of the French national transcatheter aortic-valve implantation registry, FRANCE 2.
METHODS:
All TAVIs performed in France, as listed in the FRANCE 2 registry, were prospectively included in the study. The primary end point was death from any cause.
RESULTS:
A total of 3195 patients were enrolled between January 2010 and October 2011 at 34 centers. The mean (±SD) age was 82.7±7.2 years; 49% of the patients were women.
All patients were highly symptomatic and were at high surgical risk for aortic-valve replacement. Edwards SAPIEN and Medtronic CoreValve devices were implanted in 66.9% and 33.1% of patients, respectively. Approaches were either transarterial (transfemoral, 74.6%; subclavian, 5.8%; and other, 1.8%) or transapical (17.8%).
The procedural success rate was 96.9%. Rates of death at 30 days and 1 year were 9.7% and 24.0%, respectively.
At 1 year, the incidence of stroke was 4.1%, and the incidence of periprosthetic aortic regurgitation was 64.5%.
In a multivariate model, a higher logistic risk score on the European System for Cardiac Operative Risk Evaluation (EuroSCORE), New York Heart Association functional class III or IV symptoms, the use of a transapical TAVI approach, and a higher amount of periprosthetic regurgitation were significantly associated with reduced survival.
CONCLUSIONS:
This prospective registry study reflected real-life TAVI experience in high-risk elderly patients with aortic stenosis, in whom TAVI appeared to be a reasonable option.
Rutger-Jan Nuis, MSc, Nicolas M. Van Mieghem, MD, Carl J. Schultz, MD, PhD, Adriaan Moelker, MD, PhD , Robert M. van der Boon, MSc, Robert Jan van Geuns, MD, PhD, Aad van der Lugt, MD, PhD, Patrick W. Serruys, MD, PhD, Josep Rodés-Cabau, MD, Ron T. van Domburg, PhD, Peter J. Koudstaal, MD, PhD, Peter P. de Jaegere, MD, PhD. Frequency and Causes of Stroke During or After Trans-catheter Aortic Valve Implantation.American Journal of Cardiology Volume 109, Issue 11 , Pages 1637-1643, 1 June 2012 [full abstract provided].
Transcatheter aortic valve implantation (TAVI) is invariably associated with the risk of clinically manifest transient or irreversible neurologic impairment. We sought to investigate the incidence and causes of clinically manifest stroke during TAVI. A total of 214 consecutive patients underwent TAVI with the Medtronic-CoreValve System from November 2005 to September 2011 at our institution. Stroke was defined according to the Valve Academic Research Consortium recommendations. Its cause was established by analyzing the point of onset of symptoms, correlating the symptoms with the computed tomography-detected defects in the brain, and analyzing the presence of potential coexisting causes of stroke, in addition to a multivariate analysis to determine the independent predictors. Stroke occurred in 19 patients (9%) and was major in 10 (5%), minor in 3 (1%), and transient (transient ischemic attack) in 6 (3%). The onset of symptoms was early (≤24 hours) in 8 patients (42%) and delayed (>24 hours) in 11 (58%). Brain computed tomography showed a cortical infarct in 8 patients (42%), a lacunar infarct in 5 (26%), hemorrhage in 1 (5%), and no abnormalities in 5 (26%). Independent determinants of stroke were new-onset atrial fibrillation after TAVI (odds ratio 4.4, 95% confidence interval 1.2 to 15.6), and baseline aortic regurgitation grade III or greater (odds ratio 3.2, 95% confidence interval 1.1 to 9.3).
In conclusion, the incidence of stroke was 9%, of which >1/2 occurred >24 hours after the procedure. New-onset atrial fibrillation was associated with a 4.4-fold increased risk of stroke. In conclusion, these findings indicate that improvements in postoperative care after TAVI are equally, if not more, important for the reduction of peri-procedural stroke than preventive measures during the procedure.
Sinning JM, Hammerstingl C, Vasa-Nicotera M, Adenauer V, Lema Cachiguango SJ, Scheer AC, Hausen S, Sedaghat A, Ghanem A, Müller C, Grube E,Nickenig G, Werner N. (2012). Aortic regurgitation index defines severity of peri-prosthetic regurgitation and predicts outcome in patients after transcatheter aortic valve implantation. J Am Coll Cardiol. 2012 Mar 27;59(13):1134-41. [full abstract provided].
OBJECTIVES:
The aim of this study was to provide a simple, reproducible, and point-of-care assessment of peri-prosthetic aortic regurgitation (periAR) during trans-catheter aortic valve implantation (TAVI) and to decipher the impact of this peri-procedural parameter on outcome.
BACKGROUND:
Because periAR after TAVI might be associated with adverse outcome, precise quantification of periAR is of paramount importance but remains technically challenging.
METHODS:
The severity of periAR was prospectively evaluated in 146 patients treated with the Medtronic CoreValve (Minneapolis, Minnesota) prosthesis by echocardiography, angiography, and measurement of the aortic regurgitation (AR) index, which is calculated as ratio of the gradient between diastolic blood pressure (DBP) and left ventricular end-diastolic pressure (LVEDP) to systolic blood pressure (SBP): [(DBP – LVEDP)/SBP] × 100.
RESULTS:
After TAVI, 53 patients (36.3%) showed no signs of periAR and 71 patients (48.6%) showed only mild periAR, whereas 18 patients (12.3%) and 4 patients (2.7%) suffered from moderate and severe periAR, respectively. The AR index decreased stepwise from 31.7 ± 10.4 in patients without periAR, to 28.0 ± 8.5 with mild periAR, 19.6 ± 7.6 with moderate periAR, and 7.6 ± 2.6 with severe periAR (p < 0.001), respectively. Patients with AR index <25 had a significantly increased 1-year mortality risk compared with patients with AR index ≥25 (46.0% vs. 16.7%; p < 0.001). The AR index provided additional prognostic information beyond the echocardiographically assessed severity of periAR and independently predicted 1-year mortality (hazard ratio: 2.9, 95% confidence interval: 1.3 to 6.4; p = 0.009).
CONCLUSIONS:
The assessment of the AR index allows a precise judgment of periAR, independently predicts 1-year mortality after TAVI, and provides additional prognostic information that is complementary to the echocardiographically assessed severity of periAR.
Gotzmann M, Lindstaedt M, Mügge A. (2012). From pressure overload to volume overload: Aortic regurgitation after transcatheter aortic valve implantation. Am Heart J. 2012 Jun;163(6):903-11. [full abstract provided].
Severe aortic valve stenosis is a common valvular heart disease that is characterized by left ventricular (LV) pressure overload. A lasting effect of pressure overload is LV remodeling, accompanied by concentric hypertrophy and increased myocardial stiffness. Transcatheter aortic valve implantation (TAVI) has emerged as an alternative to surgical aortic valve replacement for patients with severe symptomatic aortic valve stenosis and high surgical risk. Although TAVI has favorable hemodynamic performance, aortic valve regurgitation (AR) is the most frequent complication because of the specific technique used for implantation of transcatheter valves.
During implantation, the calcified native valve is pushed aside, and the prosthesis usually achieves only an incomplete prosthesis apposition. As a consequence, the reported prevalence of moderate and severe AR after TAVI is 6% to 21%, which is considerably higher than that after a surgical valve replacement. Although mild AR probably has minor hemodynamic effects, even moderate AR might result in serious consequences. In moderate and severe AR after TAVI, a normal-sized LV with increased myocardial stiffness has been exposed to volume overload. Because the noncompliant LV is unable to raise end-diastolic volume, the end-diastolic pressure increases, and the forward stroke volume decreases. In recent years, an increasing number of patients have successfully undergone TAVI. Despite encouraging overall results, a substantial number of patients receive neither symptomatic nor prognostic benefits from TAVI. Aortic valve regurgitation has been considered a potential contributor to morbidity and mortality after TAVI. Therefore, various strategies and improvements in valve designs are mandatory to reduce the prevalence of AR after TAVI.
Walther T , Thielmann M, Kempfert J, Schroefel H, Wimmer-Greinecker G, Treede H, Wahlers T, Wendler O. (2012). PREVAIL TRANSAPICAL: multicentre trial of transcatheter aortic valve implantation using the newly designed bioprosthesis (SAPIEN-XT) and delivery system (ASCENDRA-II). Eur J Cardiothorac Surg. 2012 Aug;42(2):278-83. Epub 2012 Jan 30. [full abstract provided].
OBJECTIVE
Transapical (TA- aortic valve implantation (AVI) has evolved as an alternative procedure for high-risk patients. We evaluated the second-generation SAPIEN xt ™ prosthesis in a prospective multicentre clinical trial.
METHODS
A total of 150 patients (age : 81.6; 40.7 % female) were included. Prosthetic valves (diameter :23 mm (n= 36), 26 mm (n= 57) and 29 mm (n= 57) were implanted. The ASCENDRA-II™ modified delivery system was used in the smaller sizes. Mean logistic EuroSCORE was 24.3% and mean STS score was 7.5 ± 4.4%. All patients gave written informed consent.
RESULTS:
Off-pump AVI was performed using femoral arterial and venous access as a safety net. All but two patients receivec TA-AVI, as planned. The 29-mm valve showed similar function as the values of two other diameters did. Three patients (2%) required temporary bypass support.
Postoperative complications included renal failure requiring long-term dialysis in four, bleeding requiring re-thoracotomy in four, respiratory complication requiring re-intubation in eight and septsis in four patients, respectively.
Thirty day mortality was 13 ( 8.7%) for the total cohort and 2/57 (3.5%) receiving the 29 mm valve respectively. Echocardiography at discharge showed none or trivial incompetence (AI) in 71% and mild-AI in 22% of the patients. Post-implantation AI was predominantly para-valvular and > 2+ in 7% of patients. One patient required re-operation for AI within 30 days.
CONCLUSION
The PREVAIL TA multicenter trial demonstrates good functionality and good outcomes for TA-AVI, using the SAPIEN xt ™ and its second generation ASCENDRA-II™ delivery system, as well successful introduction of the 29-mm SAPIEN XT ™ valve for the benefit of high-risk elderly patients.
Subramanian S, Rastan AJ, Holzhey D, Haensig M, Kempfert J, Borger MA, Walther T, Mohr FW. (2012). Conventional Aortic Valve Replacement in Transcatheter Aortic Valve Implantation Candidates: A 5-Year Experience. Ann Thorac Surg. July 19 2012 [full abstract provided].
BACKGROUND:
Patient selection for transcatheter aortic valve implantation (TAVI) remains highly controversial. Some screened patients subsequently undergo conventional aortic valve replacement (AVR) because they are unsuitable TAVI candidates. This study examined the indications and outcomes for these patients, thereby determining the efficacy of the screening process.
METHODS:
Between January 2006 and December 2010, 79 consecutive patients (49% men), aged older than 75 years with high surgical risk, were screened for TAVI, but subsequently underwent conventional AVR through a partial or complete sternotomy. The indications, demographics, and outcomes of this cohort were studied.
RESULTS:
Mean age was 80.4 ± 3.6 years. Mean left ventricular ejection fraction was 0.55 ± 0.16, and the mean logistic European System for Cardiac Operative Risk Evaluation was 13% ± 7%. Of the 79 patients, 6 (7.6%) had prior cardiac surgical procedures. Indications for TAVI denial after patient evaluations were a large annulus in 31 (39%), acceptable risk profile for AVR in 24 (30%), need for urgent operation in 11 (14%), and concomitant cardiovascular pathology in 5 (6%). Mean cross-clamp time was 55 ± 14 minutes, and cardiopulmonary bypass time was 81 ± 21 minutes. Concomitant procedures included a Maze in 12 patients (15%). Postoperative morbidity included permanent stroke in 2 (2.5%), respiratory failure in 9 (11%), and pacemaker implantation in 2 (2.5%). Hospital mortality was 1.3% (1 of 79). Cumulative survival at 6, 12, and 36 months was 88.5%, 87.1% and 72.7%, respectively.
CONCLUSIONS:
Our existing patient evaluation process accurately defines an acceptable risk cohort for conventional AVR. The late mortality rate reflects the advanced age and comorbidities of this cohort. The data suggest that overzealous widening of TAVI inclusion criteria may be inappropriate.
Industry fights back
Now it looks like Edwards Lifesciences, the company that manufacturers the Sapien valve is speaking out to dispute recent findings that show TAVI to have less than optimal results. Of course, the author at the site, Med Latest says it best, “Setting aside the conflict of interest stuff, which might be a red-herring, what we’re left with is a situation where evidence-based medicine, while being something all would sign up to, is not that straightforward.”
[1] Several cardiologists and cardiac surgeons contributed to this article. However, given the current politics within cardiology, none of these experts were willing to risk their reputations by publically disputing the majority opinion. This is certainly understandable in today’s medico-legal climate in wake of widespread scandals and credibility issues. However, all quotes are accurate, even if unattributable with minor formatting (such as the addition of quotations, and paragraph headings have been added for increased clarity of reading in blog format.) I apologize for the ‘anonymous nature’ of my sources in this instance – however, I can assure you that these ‘experts’ know what they are talking about.
[All commentary by Cartagena Surgery are in italics and brackets].
Thanks again to ‘Lapeyre’, who as it turns out is Dr. Didier Lapeyre, a renowned, French cardiothoracic surgeon credited with the development of the first mechanical valves.
Dr. Didier Lapeyre was gracious enough to send some additional literature to add to our ongoing discussions regarding severe aortic stenosis and TAVI/ TAVR therapies. He also commented that the best way to avoid these ‘high risk situations’ is by earlier intervention with conventional surgery – something we discussed before in the article entitled, “More patients need surgery.”
He also points out that ‘elderly’ patients actually do quite well with aortic valve replacement and offers a recently published meta-analysis of 48 studies on patients aged 80 or older.
As readers know, on June 13, 2012 – the FDA ruled in favor of expanding the eligibility criteria for this therapy. Previously, this treatment modality, due to its experimental nature and high rate of complications including stroke and serious bleeding, has been limited in the United States to patients deemed ineligible for aortic valve replacement surgery.
Now on the heels of the Partner A trial, in which researchers reported favorable results for patients receiving the Sapien device, the FDA has voted to approve expanding criteria to include patients deemed to be high risk candidates for surgery. As we have discussed on previous occasions, this opens the door to the potential for widespread abuse, misapplication of this therapy and potential patient harm.
Most notably, is the evidence of widespread abuse in Germany (page 49 of report), which has become well-known for their early adoption of this technology, and now uses TAVI for an estimated 25 – 40% of valve procedures*. Closer examination of the practices in this country show poor data reporting with incomplete information in the national registry as well as a reported mortality rate of 7.7%, which is more than double that of conventional surgery. Unsurprisingly, in Germany, TAVI is reimbursed at double the amount compared to conventional surgery**, providing sufficient incentive for hospitals and cardiologists to use TAVI even in low risk patients. (and yes, german cardiologists are often citing “patient refused surgery” as their reason, particularly when using TAVI on younger, healthy, low risk patients.)
In their examination of the data itself, Mattias et al. (2011) found significant researcher bias within the study design and interpretation of results. More alarmingly, Mattias found that one of the principle researchers in the Partner A study, Dr. Martin Leon had major financial incentives for reporting successful results. He had recently received a 6.9 million dollar payment from Edward Lifesciences, the creators of the Sapien valve for purchase of his own transcatheter valve company. He also received 1.5 million dollar bonus if the Partner A trial reached specific milestones. This fact alone, in my mind, calls into question the integrity of the entire study.
[Please note that this is just a tiny summary of the exhaustive report.]
Thank you, Dr. Lapeyre for offering your expertise for the benefit of our readers!
* Estimates on the implantation of TAVI in Germany vary widely due to a lack of consistent reporting.
** At the time of the report, TAVI was reimbursed at 36,000 euros (45,500 dollars) versus 17,500 euros (22,000 dollars) for aortic valve replacement.
For more posts on TAVI and aortic stenosis, see our TAVI archive.
As reported by heartwire, and a savvy reader, Lapeyre here at Cartagena Surgery, the FDA has gone ahead and approved TAVI/ TAVR for patients that are eligible for open surgery. [We must think alike, as I was drafting this post when I received the reader mail].
Despite the FDA’s previously cited concerns over the excessive stroke rate with the Sapien device (as discussed in the article re-posted below) – the FDA approved the use of this therapy as an alternative to surgery on June 13th.
Now we can sit back and watch as the up selling of this device to the public as news hits the US media and the television advertisements begin. Soon this device will crowd out surgery as interventionalists cite “patient refused surgery” as the criteria for implantation, no matter what the best interest of the patient really is. I wonder if they will even disclose the heightened stroke rate when they start implanting this into patients at a much higher rate. Of the 12 members of the FDA panel, only one member voted against the expansion criteria.
As reported by Shelley Wood in a follow-up Heartwire article , only Dr Valluvan Jeevanandam spoke out against expanding the criteria for use, stating, “I think this is a very good technology, and it gives us an alternative to AVR surgery, and I’m sure the device will continue to get better,” Jeevanandam, a cardiovascular surgeon, told heartwire after the meeting.
“However, at the current time, compared with standard AVR, this device has a higher stroke rate and a high rate of aortic insufficiency, did not meet the criteria for noninferiority* in males, and has a high incidence of vascular complications.”
These are all issues that need to be very clearly explained to patients as part of the informed-consent process, he stressed. Otherwise, patients who are “enamored at the idea of avoiding a sternotomy” may not fully understand these risks.”
I fully concur with Dr. Valluvan Jeevanandam except that I might re-phase the term ‘enamored of.’ Actually, I think our so-called peers need to quit coercing patients by intentionally scaring them – in order to bill more procedures out of them. [Don’t believe it? Then check out Mark Midei and our overstenting archives.]
I will continue to champion well-established therapies with strong long term data. I know this will get me labeled as ‘old-fashioned’ (or worse) but as we’ve seen in cardiology – numerous times; easy is not always the best answer..
Yes, conventional surgery hurts – it’s not glamorous, it’s not pretty. But it’s (statistically) darn safe these days, and most of the surgeons doing it have done it thousands of times.. Even the bioprosthetic valves have a long durability than previously thought – meaning not everyone has to take warfarin..
We shouldn’t exploit people’s fears of surgery to use quasi-experimental procedures, no matter how “cool” they sound..
* I hope readers remember that ‘noninferiority’ is a lesser standard that superior to, or even EQUAL to..
FDA flags strokes, trial conduct, as TAVI maker seeks expanded role for Sapien – from Heartwire.com (Shelley Wood).
Gaithersburg, MD – A higher risk of stroke and differences in how patients randomized to different procedures were actually treated and evaluated within the PARTNER A trial, which compared transcatheter aortic-valve implantation (TAVI) with surgery, are issues the US Food and Drug Administration (FDA) hopes its expert advisors can help clarify in weighing the pros and cons of expanding approval of the Sapien transcatheter valve (Edwards Lifesciences) [1,2]. Those issues and others are detailed in an FDA briefing document, posted online today, that the agency’s Circulatory System Devices Panel will consider in advance of Wednesday’s meeting.
As previously reported by heartwire, the FDA last year reviewed and subsequently approved the Sapien valve and transfemoral delivery system in patients not suited to open-valve replacement, based primarily on the PARTNER B results. Wednesday’s meeting, drawing heavily on the PARTNER A results, will help the FDA decide whether to expand approval to high-risk patients who are surgery eligible and whether to approve the transapical approach also tested in PARTNER A.
In briefing documents posted online today, the FDA directed its advisors to pay special attention to a number of issues relating to trial conduct as well as patient outcomes.
In particular, the FDA review cites the “doubling” of neurological events seen in the Sapien-treated patients in the first 30 days postprocedure, with a higher stroke rate seen among transapical as compared with the transfemoral group.
The FDA documents also query “attempt-to-treat” decisions, including the higher number of patients randomized to surgery in whom no treatment was attempted; longer delays to treatment in surgical patients; and the higher number of concomitant operations seen in the surgical aortic-valve-replacement group—all factors that could have influenced adverse-event and survival rates in this group.
FDA is also asking its expert panel to weigh in on whether both the transfemoral and transapical approaches should be approved, given the numerically higher mortality in the transapically treated patients as compared with the transfemorally treated patients in the device arm.
General questions the FDA panel will be answering Wednesday include those related to the issues above, as well as to different outcomes seen in men and women, the importance of paravalvular regurgitation seen in patients treated with TAVI, valve durability, the required anticoagulation/antiplatelet regimen, and obtaining true informed consent.
Voting questions center on whether the evidence is sufficient to demonstrate safety and efficacy and whether the benefits of the new device outweigh the risks.
Industry analysts reading the tea leaves in the FDA’s review see the agency’s briefing document as largely promising, with Wells Fargo’s Larry Biegelsen predicting a “tough day, but positive panel outcome” and JP Morgan’s Michael Weinstein stating that the FDA synopsis contained “no major surprises; positive outcome expected.”
In other cardiology news,
New guidelines recommend the discontinuation of prasugrel a full seven days before surgery to prevent catastrophic bleeding complications. (The cynical side of me expects to see a bigger push by the industry to use prasugrel now that clopidogrel is generic.) Expect to see a couple more “Ask your doctor” ads..
No – I haven’t changed the name of the blog, just reflecting the nature of my current assignment. Spending some time in Interventional Cardiology this week as part of a story I am writing about chest pain emergencies for Mexico on my mind.com. Today, I checked out the cath lab at Hispano Americano Hospital. It’s a bit crowded, but all the equipment is brand-spanking new, and practically sparkling. (Don’t worry – I have photos to prove it!)
Nurses in the cath lab at Hospital Hispano Americano
Dr. Fernando Monge was kind of enough to give me a guided tour. While we were there he (assisted by Dr. Raul Aguilera) placed a stent in a patient with recurrent angina. A doctor from the ER also stopped by to have him review a couple EKGs.. I’ll post a link when the full story is done.
Also stopped in to talk to Dr. Jose Antonio Olivares Felix, MD, a general surgeon who reports to me that he is doing single port laparoscopy – so of course, that got me interested. Hoping to set a date to go to the operating room.
I’ll be spending all of tomorrow in the company of Dr. Marnes Molina, MD to learn more about some of the other stuff he’s doing in urology (and hopefully grab a picture of that green laser!)
Note: I owe Dr. Vasquez a much more detailed article – which I am currently writing – but after our intellectually stimulating talk the other day, my mind headed off in it’s own direction..
Had a great sit down lunch and a fascinating talk with Dr. Vasquez. As per usual – our discussion was lively, (a bit more lively than usual) which really got my gears turning. Dr. Vasquez is a talented surgeon – but he could be even better with just a little ‘help’. No – I am not trying to sell him a nurse practitioner – instead I am trying to sell Mexicali, and a comprehensive cardiac surgery program to the communities on both sides of the border.. Mexicali really could be the ‘land of opportunity’ for medical care – if motivated people and corporations got involved.
During lunch, Dr. Vasquez was explaining that there is no real ‘heart hospital’ or cardiac surgery program, per se in Mexicali – he just operates where ever his patients prefer. In the past that has included Mexicali General, Issstecali (the public hospitals) as well as the tiny but more upscale private facilities such as Hospital Alamater, and Hospital de la Familia..
Not such a big deal if you are a plastic surgeon doing a nip/tuck here and there, or some outpatient procedures – okay even for general surgeons – hernia repairs and such – but less than ideal for a cardiac surgeon – who is less of a ‘lone wolf’ due to the nature and scale of cardiac surgery procedures..
Cardiac surgery differs from other specialties in its reliance on a cohesive, well-trained and experienced group – not one surgeon – but a whole team of people to look out for the patients; Before, During & After surgery.. That team approach [which includes perfusionists, cardiac anesthesiologists (more specialized than regular anesthesia), operating room personnel, cardiology interventionalists and specialty training cardiac surgery intensive care nurses] is not easily transported from facility to facility.
just a couple members of the cardiac surgery team
That’s just the people involved; it doesn’t even touch on all the specialty equipment; such as the bypass pump itself, echocardiogram equipment, Impella/ IABP (intra-aortic balloon pump), ECMO or other equipment for the critically ill – or even just the infrastructure needed to support a heart team – like a pharmacy division that knows that ‘right now’ in the cardiac OR means five minutes ago, or a blood bank with an adequate stock of platelets, FFP and a wide range of other blood products..
We haven’t even gotten into such things such as a hydrid operating rooms and 24/7 caths labs – all the things you need for urgent/ emergent cases, endovascular interventions – things a city the size of Mexicali should really have..
But all of those things take money – and commitment, and I’m just not sure that the city of Mexicali is ready to commit to supporting Dr. Vasquez (and the 20 – something cases he’s done this year..) It also takes vision..
This is where a company/ corporation could come in and really change things – not just for Dr. Vasquez – and Mexicali – but for California..
It came to me again while I was in the operating room with Dr. Vasquez – watching him do what he does best – which is sometimes when I do what I do best.. (I have some of my best ideas in the operating room – where I tend to be a bit quieter.. More thinking, less talking)..
Dr. Vasquez, doing what he does best..
As I am watching Dr. Vasquez – I starting thinking about all the different cardiac surgery programs I’ve been to: visited, worked in – trained in.. About half of these programs were small – several were tiny, single surgeon programs a lot like his.. (You only need one great surgeon.. It’s all the other niceties that make or break a program..)
All of the American programs had the advantages of all the equipment / specialty trained staff that money could buy***
[I know what you are thinking – “well – but isn’t it all of these ‘niceties’ that make everything cost so darn much?” No – actually it’s not – which is how the Cardioinfantils, and Santa Fe de Bogotas can still make a profit offering world-class services at Colombian prices…]
The cost of American programs are inflated due to the cost of defensive medicine practices (and lawyers), and the costs of medications/ equipment in the United States****
the possibilities are endless – when I spend quality time in the operating room (thinking!)
Well – there is plenty of money in Calexico, California** and not a hospital in sight – just a one room ‘urgent care center’. The closest facility is in El Centro, California – and while it boasts a daVinci robot, and a (part-time?) heart surgeon (based out of La Mesa, California – 100 + miles away)– patients usually end up being transferred to San Diego for surgery.
Of course, in addition to all of the distance – there is also all of the expense.. So what’s a hard-working, blue-collar guy from Calexico with severe CAD going to do? It seems the easiest and most logical thing – would be to walk/ drive/ head across the street to Mexicali.. (If only Kaiser Permanente or Blue Cross California would step up and spearhead this project – we could have the best of both worlds – for residents of both cities..
A fully staffed, well-funded, well-designed, cohesive heart program in ONE medium- sized Mexicali facility – without the exorbitant costs of an American program (from defensive medicine practices, and outlandish American salaries.) Not only that – but as a side benefit, there are NO drug shortages here..
How many ‘cross-border’ cases would it take to bring a profit to the investors? I don’t know – but I’m sure once word got out – people would come from all over Southern California and Arizona – as well as Mexicali, other parts of Baja, and even places in Sonora like San Luis – which is closer to Mexicali than Hermasillo.. Then Dr. Vasquez could continue to do what he does so well – operate – but on a larger scale, without worrying about resources, or having to bring a suitcase full of equipment to the OR.
The Mexican – American International Cardiac Health Initiative?
But then – this article isn’t really about the ‘Mexican- American cross-border cardiac health initiative’ –
It is about a young, kind cardiac surgeon – with a vision of his own.
That vision brought Dr. Vasquez from his home in Guadalajara (the second largest city in Mexico) to one of my favorite places, Mexicali after graduating from the Universidad Autonomica in Guadalajara, and completing much of his training in Mexico (D.F.). After finishing his training – Dr. Vasquez was more than ready to take on the world – and Mexicali as it’s first full-time cardiac surgeon.
Mexicali’s finest: Dr. Vasquez, (cardiac surgeon) Dr. Campa(anesthesia) and Dr. Ochoa (thoracic surgeon
Since arriving here almost two years ago – that’s exactly what he’s done.. Little by little, and case by case – he has begun building his practice; doing a wide range of cardiovascular procedures including coronary bypass surgery (CABG), valve replacement procedures, repair of the great vessels (aneurysm/ dissections), congenital repairs, and pulmonary thrombolectomies..
Had a great day in the operating room with Dr. Cuauhtemoc Vasquez, MD the promising young heart surgeon I told you about several months ago. I have some absolutely breathtaking photos of the case – but I want to double-check with the patient before posting anything potentially revealing in such a public forum.
Todays’ surgery was at one of the public hospitals in Mexicali – and while technology was sometimes in short supply – talent sure wasn’t. I was frankly surprised at the level of skill and finesse Dr. Vasquez displayed given the fact that he is so early in his career.
Dr. Cuauhtemoc Vasquez, Cardiac surgeon
He’s also just an all-around pleasant and charming person. I know from previous encounters that he’s well-spoken, interesting, engaging and an excellent conversationalist – We didn’t talk at length on this occasion – because honestly, I really don’t like to be distracting during cases – especially since much of the discussion was in an English-heavy Spanglish.. (He is fluent in English but we both tend to slip in and out of Spanish. I mainly slip out when I start thinking in English and come across a concept that I am not sure about explaining or asking about in Spanish.**
But don’t worry – I am planning on seeing him next week – where I can hopefully lure him to lunch/ coffee or something so we have a more lengthy discussion – so I can give you all the details in a more formal fashion in a future post.
As a crazy side note – finally got that ‘great’ picture of the good doctor.. Oh, the irony – not during a thoracic case but while he was assisting Dr. Vasquez – (the good doctor is board-certified cardiothoracic surgeon, after all..) I didn’t post it here because there are some ‘patient bits’ in the photo..
**I know this can be frustrating from my experiences with my professor – but it’s also frustrating when: a. a question gets misinterpreted as a statement (because of my poor grammar) or b. misconstrued completely – which still happens pretty frequently. Luckily, people around here are awfully nice, and tend to give me the benefit of a doubt.
Also – I need to post this photo of one of my favorite operating room nurses – Lupita. (Lupita along with Carmen and Marisol) have been an absolute delight to be around even of those very first anxious days..
Lupita, operating room nurse.. Doesn’t hurt that she’s as cute as a button, eh?
with Dr. Pulido (left) and Dr. Barbosa in Cartagena (2010).
I wanted to post an update on a fantastic surgeon (who has since become a good friend). In fact, Dr. Cristian Barbosa was one of the first surgeons I ever interviewed back in 2010 – and without his encouragement, the first book would have never gotten off the ground. Maybe not the second book (Bogotá!) either – since once I said the magic words, “Oh – I interviewed Dr. Barbosa in Cartagena last year,” plenty of other surgeons who might not have talked to me – started to take me seriously.
with Dr. Barbosa back in 2010
Ever since then – I try to keep in contact with Dr. Barbosa – he’s a great person and an absolutely phenomenal surgeon, so I email him every so often..
Since my last visit, back in August – Dr. Barbosa has left Hospital Neuvo Bocagrande – and is now operating in Clinica Santa Maria in Sincelejo, Colombia.
Sincelejo is the capital of the state of Sucre, which is part of the Caribbean region of Colombia. Like most of this part of Colombia – it has a rich history, and was founded back in 1535 in the name of St. Francis de Assis, though it was long inhabited prior to that by native Colombian tribes such as the Zenu. Unlike nearby Cartagena (125km north), Sincelejo is a more mountainous landscape, and is known for their agriculture, particularly cattle. (wow – my stomach just rumbled – must be missing those gourmet Corral burgers, which are my one Colombian indulgence.. Argentina has nothing on Colombian beef.)
Dr. Barbosa is still living in Cartagena and making a three-hour commute to perform life-saving surgery, while he works on creating a new cardiac surgery program back in our favorite seaside city. (Hopefully, when he does – we’ll be invited back to take a look!)
Not as innocent as the Corn Refiners Association would have you believe.
In a courtroom in Los Angeles, a fierce battle is being pitched right now – one that affects almost every person in this nation.. It’s a lawsuit from the nation’s sugar producers accusing the corn industry of false advertising.. That’s right – it takes industry giants to take on those ridiculous, and mis-leading ads.
But, here (finally) is a response to those ads – that uses science, not fallacy to refute those claims.
At the same time, the Corn Refiners Association has filed a petition with the Food & Drug Administration to change the name of their product from ‘High-fructose corn syrup” to the more innocuous-sounding “Corn Sugar,” which is just another attempt to deceive the American public.
Unfortunately, corn syrup in our everyday products in not usually so easy to identify.
A soda a day raises CHD risk by 20% – Lisa Nainggolan
March 12. 2012
Boston, MA – Sugary drinks are associated with an increased risk of coronary heart disease (CHD) as well as some adverse changes in lipids, inflammatory factors, and leptin, according to a new analysis of men participating in the Health Professionals Follow-up Study, reported by Dr Lawrence de Koning (Children’s Hospital Boston, MA) and colleagues online March 12, 2012 in Circulation [1].
“Even a moderate amount of sugary beverage consumption—we are talking about one can of soda every day—is associated with a significant 20% increased risk of heart disease even after adjusting for a wide range of cardiovascular risk factors,” senior author Dr Frank B Hu (Harvard School of Public Health, Boston, MA) told heartwire. “The increased risk is quite substantial, and I think has important public-health implications given the widespread consumption of soda, not only in the US but also increasing very rapidly in developing countries.”
The increased risk is quite substantial, and I think has important public-health implications given the widespread consumption of soda.
The researchers did not find an increased risk of CHD with artificially sweetened beverages in this analysis, however. “Diet soda has been shown to be associated with weight gain and metabolic diseases in previous studies, even though this hasn’t been substantiated in our study,” says Hu. “The problem with diet soda is its high-intensity sweet taste, which may condition people’s taste. It’s still an open question whether diet soda is an optimal alternative to regular soda; we need more data on this. ”
Hu says water is the best thing to drink, or coffee or tea. Fruit juice is “not a very good alternative, because of the high amount of sugar,” he adds, although if diluted with water, “it’s much better than a can of soda,” he notes.
And Hu says although the current results apply only to men, prior data from his group in women in the Nurses’ Health Study [from 2009] were comparable, “which really boosts the credibility of the findings.”
Inflammation could be a pathway for impact of soda upon CHD risk
Hu and colleagues explain that while much research has shown a link between the consumption of sugar-sweetened beverages and type 2 diabetes, few studies have looked at the association of these drinks with CHD.
Hence, they analyzed the associations of cumulatively averaged sugar-sweetened (eg, sodas) and artificially sweetened (eg, diet sodas) beverage intake with incident fatal and nonfatal CHD (MI) in 42 883 men in the Health Professionals Follow-up study. Beginning in 1986 and every two years until December 2008, participants answered questionnaires about diet and other health habits. A blood sample was provided midway through the study.
There were 3683 CHD cases over 22 years of follow-up. Those in the top quartile of sugar-sweetened-beverage intake had a 20% higher relative risk of CHD than those in the bottom quartile (RR 1.20; p for trend <0.001) after adjustment for age, smoking, physical activity, alcohol, multivitamins, family history, diet quality, energy intake, body-mass index, preenrollment weight change, and dieting.
Adjustment for self-reported high cholesterol, high triglycerides, high blood pressure, and diagnosed type 2 diabetes only slightly attenuated these associations, which suggests that drinking soda “may impact on CHD risk above and beyond traditional risk factors,” say the researchers.
Consumption of artificially sweetened drinks was not significantly associated with CHD (multivariate RR 1.02; p for trend=0.28).
Intake of sugar-sweetened drinks, but not artificially sweetened ones, was also significantly associated with increased triglycerides and several circulating inflammatory factors—including C-reactive protein, interleukin 6 (IL-6), and tumor-necrosis-factor receptor 1 (TNFr1)—as well as decreased HDL cholesterol, lipoprotein (a) (Lp[a]), and leptin (p<0.02).
“Inflammation is a key factor in the pathogenesis of cardiovascular disease and cardiometabolic disease and could represent an additional pathway by which sugar-sweetened beverages influence risk,” say Hu et al.
Cutting consumption of soda is one of easiest behaviors to change
Hu says that one of the major constituents of soda, high-fructose corn syrup, is subsidized in the US, making such drinks “ridiculously cheap” and helping explain why consumption is so high, particularly in lower socioeconomic groups.
Doctors should be advising people with heart disease or at risk to cut back on sugary beverages; it’s almost a no-brainer.
“Doctors should set an example for their patients first,” he stresses. “Then, for people who already have heart disease or who are at high risk, physicians should be advising them to cut back on sugary beverages; it’s almost a no-brainer, like recommending that they stop smoking and do more exercise. The consumption of sugary beverages is a relatively easy behavior to change.”
And although this particular study included mostly white subjects and there are few data on the risk of cardiovascular disease associated with the consumption of soda in people of other ethnicities, there are data on its effect on type 2 diabetes in these groups, he says.
“It has been shown for minority groups—such as African Americans and Asians—that they are more susceptible to the detrimental effects” of sugary drinks on diabetes incidence, he notes.
Busy day today – I am giving a talk with the local Mended Hearts chapter as part of “Heart Month.” Mended Hearts is a patient-run organization/ support group for people who have had heart attacks, stents or heart surgery. It’s a place where people can go for encouragement, education or support after a life-changing cardiac event. I’ve worked with Mended Hearts in the past, so I was pleased when they invited me to give one of my favorite talks this weekend. (I’ve been giving variations on this talk since 2008).
(Some people might consider it a bit ironic that I am giving a lecture on prevention to a group of people who have already been diagnosed with CAD – but we are also talking about overall wellness/ and preventing future events.)
It’s one of my favorite lectures because it’s an informal style presentation – so I encourage listeners to participate in the discussion – and ask questions. We also review a case study at the end – where we have a bit of role reversal as I invite listeners to be the NP for a minute and devise treatment strategies for the imaginary patient.. (and my audience usually does a great job – which just proves how powerful a motivated person can be when it comes to healthcare.. If all people were like my audiences, people would be a lot healthier.) I’ve included a quick summary of my lecture here for interested readers. (Just the basics – for more specific or detailed information such as information on lipo-proteins, see your doctor.)
Aggressive Risk Factor Reduction
When talking about healthcare and risk factor reduction, we need to use measurable, and achievable goals.. No ‘nebulous’ statements like ‘improve blood pressure’, or ‘lose weight.’ Instead – we give concrete, and specific goals based on the most relevant and up-to-date clinical evidence.
1. Hypertension / Blood pressure control – normal B/P is 110/ 70. National guidelines for diabetics recommends systolic blood pressure less than 130, and a diastolic b/p less than 90.
– statin therapy recommended for all diabetics. 3. Microaluminuria – small protein particles found in urine. This is an early indicator of on-going kidney damage. All diabetics should be on an ace-inhibitor (the ‘prils’ such as lisinopril, fosinopril, enalapril).
These medications will help SLOW the damage, but the best treatment is TIGHT glucose control.
4. Hyperglycemia – (not diabetes)
Hyperglycemia causes damage. Period. This includes so-called ‘pre-diabetes’ and gestational diabetes (see slides for more information.)
– Check your hemoglobin A1c, and control your glucose
– Fasting and post-prandial (2 hours after meals) glucose testing. Remember that post-prandial readings will rise earlier in the course of the disease, so if you re only testing in the mornings – you might miss crucial information needed for your treatment.
– Currently ONLY metformin and insulin therapies have been shown to have long-term benefits. (The twenty – plus other medications may make ‘the numbers’ look pretty – but there is little long-term evidence to support their use.
5. Endothelial inflammation – hyperglycemia ‘encourages’ endothelial inflammation and vascular damage (it’s the hallmark of the disease) so the best way to treat this is with anti-platelet therapy such as a baby aspirin (ASA). Recent literature suggests that ASA may do more harm than good in some people, so check with your doctor..
There’s a lot more information to go over (it’s a 45 minute talk) so I’ve decided to post my lecture slides here for anyone to use, but I do ask that people please give appropriate credit. Cardiac Complications of Diabetes ppt slides.
Sat down today with Dr. Kevin Brady to talk about TAVI, or as he corrects me with a smile, TAVR (R is for Replacement). Dr. Brady is a cardiothoracic surgeon, and one of the few currently performing TAVI/ TAVR here in Arizona. As we’ve discussed before, I have mixed feelings on this procedure but have elected to provide the information here for my interested readers.
Dr. Brady shares many of my apprehensions, that the public will come to view this currently quasi-experimental treatment for very high risk, and inoperable patients with Aortic Stenosis as a ‘easy fix’. We discuss this at length, and he reviews the current recommendations guiding the implementation of TAVR programs, and the TAVR registry with me.
As part of this discussion, I have invited Dr. Brady to write a short post here, explaining the procedure, patient selection criteria and other facts about TAVI/ TAVR. With over 41 Core-valve implantations (since March 2011, as part of the Core Valve Pivotal trial) and seven Sapien valve implantations this month, he certainly qualifies as an expert on the topic.
Dr. Brady will be able to give readers a more in-depth perspective on this procedure. As all of you know, I have taken a fairly cautious stance on this issue. (I haven’t talked him into letting me observe yet, but I am working on it.)
I just read an interesting article in the Annals of Thoracic Surgery.
Unfortunately, the full-text article is not available for free – but I did find a nice article abstract (which I’ve posted below.) It confirms some of the previous discussions we’ve had here at Cartagena Surgery on the role of surgery in Aortic Stenosis, even in ‘elderly’ patients. [I put elderly in quotes since the definition can be fairly elastic depending on who is doing the judging.]
The article below is from Medscape.com
Aortic valve replacement in the elderly: the real life.
Langanay T; Flécher E; Fouquet O; Ruggieri VG; Tour Bde L; Félix C; Lelong B; Verhoye JP; Corbineau H; Leguerrier A Department of Cardiovascular and Thoracic Surgery, University Hospital, Rennes, France.
BACKGROUND: Aortic stenosis is of concern in the elderly. Although aortic valve replacement provides good long-term survival with functional improvement, many elderly patients are still not referred for surgery because of their age. Percutaneous aortic valve implantation offers an alternative to open-heart surgery. Concerns about the management of aortic valve stenosis in the elderly will be reviewed.
METHODS: We retrospectively analyzed 1,193 consecutive aortic valve replacements, performed in octogenarians since January 2000. A total of 657 patients (55%) had at least one associated comorbidity (eg, respiratory failure) and 381 (32%) associated coronary lesions. Valve replacement was the only procedure in 883 patients (74%), and was associated with coronary revascularization in 262 cases, or with another cardiac procedure in 48 patients.
RESULTS: Overall operative mortality was 6.9% (83 of 1,193 patients); 5.5% for single replacement and 11.5% if associated with coronary artery bypass surgery. Univariate and multivariate analyses identified 11 operative risk factors related to general status, cardiologic condition, and the procedure itself: older age (p< 0.015); respiratory failure (p <0.03); aortic regurgitation (p <0.001); emergency surgery (p <0.0029); New York Heart Association class IV (p < 0.0007); right heart failure (p < 0.03); atrial fibrillation (p < 0.04); impaired ejection fraction (p < 0.001); coronary disease (p < 0.01); redo surgery (p < 0.02); associated coronary revascularization (p < 0.008).
CONCLUSIONS: Today, valve replacement has acceptable low hospital mortality, even in the elderly. Thus, older patients should not be denied surgery due to their advanced age alone. Conventional surgery remains the gold standard treatment for aortic stenosis; the decision should be made on an individual basis. If several risk factors suggest very high-risk surgery, then percutaneous valve implantation should be considered instead.
In more disturbing news:
As predicted, the unproven ‘easy option’ of TAVI is now being pursued by more low-risk patients. These lower risk patients are people who should have been encouraged to undertake the more durable, safe and proven surgical therapy [Aortic Valve Replacement.] I guess this just shows how quickly those new recommendations [for patient protection and safety] were thrown out the window.
In this article (posted below) by Kurt Ullman at Medpage Today – German researchers discuss their preliminary findings and discuss the use in low risk patients.
The bar for transcatheter aortic valve implantation (TAVI) is dropping as more lower-risk patients are undergoing the procedure and their outcomes are favorable, a single-center study from Germany found. [Unfortunately – as we’ve seen so many times in the past, and as I am finding out while preparing this presentation on the Syntax trial – studies such as this can be quite deceiving – and LONG term data is needed. – Cartagena Surgery].
When stratified by quartiles based on enrollment date, Q1 patients had higher logistic EuroSCOREs, higher Society of Thoracic Surgeons (STS) scores, and higher median N-terminal pro-B-type natriuretic peptide levels compared with those enrolled later in Q4, noted Nicolo Piazza, MD, PhD, and colleagues from the German Heart Center in Munich.
Although there were significant decreases in 30-day and six-month mortality from Q1 to Q4 in the crude analysis, after adjustments for baseline characteristics, the significant differences disappeared (HR 0.29 for 30-day mortality and HR 0.67 for six-month mortality), according to the study published online in the Journal of the American College of Cardiology.
“These results suggest that underlying comorbidities play an important role in acute and intermediate-term survival after TAVI,” the researchers wrote.
The researchers noted anecdotal information suggesting a shift toward using TAVI in patients who are less sick than those enrolled in premarket trials. Additionally, the next wave of trials involving the CoreValve (Medtronic) and the Sapien XT (Edwards Lifesciences) devices will involve intermediate to high surgical risk patients, providing “yet another indication that TAVI is being directed at the treatment of lower and lower surgical risk patients,” Piazza and colleagues wrote. [There are significant ethical considerations here which seem to be ignored – similar to criticisms of the Syntax trial – Cartagena Surgery.]
A single-center French study of low-risk TAVI patients found the procedure to be safe in this population. The study was presented at the European Society of Cardiology meeting in Paris.
The impact on this shift in patient selection was uncertain, they said, prompting a retrospective review of 420 patients who underwent TAVI at their institution from June 2007 to June 2010.
The consensus that a patient was suitable for TAVI was derived from a team that comprised cardiologists, cardiac surgeons, and anesthesiologists. This team approach is exemplified by the recent announcement that the American College of Cardiology and the Society of Thoracic Surgeons will jointly sponsor a TAVI registry to monitor the safety and efficacy of the procedure as it rolls out in the U.S.
Patients received either the CoreValve or Sapien device, the latter of which was just approved for use in the U.S. based on the PARTNER trial. PARTNER found that TAVI was as good as surgery in high-risk patients with severe aortic stenosis. [‘as good as’ – ah.. another ‘non-inferiority’ study….. view with skepticism folks..]
Researchers divided patients into four quartiles of 105 patients each. Those in Q1 were seen earlier in the study time frame than those in Q4.
Compared with Q4, Q1 patients had higher EuroSCOREs (25.4% versus 17.8%, P<0.001), STS scores (7.1% versus 4.8%, P<0.001), and NT-proBNP levels (3,495 versus 1,730 ng/dL, P<0.046).
There were significantly less transfemoral access approaches from Q1 to Q4, with a concomitant rise in transapical approaches. There also were significantly less intubations moving from Q1 to Q4, and the use of contrast significantly decreased over time.
Researchers noted that transfemoral complications decreased by 17% from Q1 to Q4 (P=0.008), but found no significant differences in the rate of stroke or transient ischemic attack or the need for a permanent pacemaker.
However, there was a shift in the later quartiles toward the treatment of younger patients with fewer comorbidities and lower surgical risk scores, Piazza and colleagues wrote.
Univariable analysis for 30-day mortality showed it was associated with age, STS score, atrial fibrillation, previous heart surgery, and previous stroke (P<0.10).
The factors associated with six-month mortality were age, logistic EuroSCORE, STS score, left ventricular ejection fraction, atrial fibrillation, previous cardiac surgery, chronic obstructive pulmonary disease, and N-terminal pro-B type natriuretic peptide (P<0.10).
Because only baseline characteristics were included, the authors noted the possibility that procedure-, operator-, or device-related factors might influence both 30-day and six-month mortality. The study is also limited by potential unmeasured confounding.
The investigators cautioned that little is known of the long-term durability of these devices should they be routinely implanted in younger patients with a longer expected life span. [especially since the lifespan of the patients these valves were designed for was six months to one year..]
Piazza is a consultant and proctor for Medtronic and CardiAQ. Other authors revealed consultant status with Medtronic and Edwards Lifesciences, or instuctors for Medtronic
Just returned from a quick trip to London, UK to interview a couple of fantastic thoracic surgeons. (You can read the interview here.)
In the meantime, a midst multiple conflicting reports regarding the use and safety of TAVI (percutaneous aortic valve replacement) the ACC and STS have finally come together to create a TAVI registry, similar to the PCI and cardiac surgery registries. The new registry will be used to track TAVI procedures and outcomes. Hopefully, by gathering information in a standardized fashion and collecting data on patient outcomes, we can finally answer the essential question surrounding TAVI: Is It Safe?
As someone who is intimately involved in the STS database – I can assure readers that if STS is involved, data collection will be extensive, cumbersome and overly complicated. (The adult cardiac surgery data collection form is fourteen pages long.) However, the database will allow doctors to identify whether complications are device related/ procedure related or operator related. (For example, are post-procedural strokes caused by the valve (device related) itself, or by the person (operator related) inserting it? It will also track 30 day mortality – and the causes of mortality. (ie. Was the death coincidental versus bleeding/ stroke/ kidney failure, etc?) The registry will also track one year outcomes – but unfortunately – the essential question – Is it Safe long-term? will remain unanswered.
In Big Pharma news – I had the good fortune to meet (and talk to at length) one of the inside investigators* for GlaxoSmithKline. He was a delightful and charming interview – and it was a fascinating inside look at the future of pharmacology, pharmacy, drug development and marketing.
As readers know – I have vilified and railed against pharmaceutical companies in the past (and most likely – will continue to do so) but it was an excellent opportunity to see the other side of a blighted industry. [Here at Cartagena Surgery – I may have unabashedly strong opinions, but I do try to be fair.]
As an investigator for a pharmaceutical company, his position is somewhat akin to George Clooney’s character in the recent film ‘Up in the Air’. He investigates company employees as well as independent contractors who represent the company for moral, ethical and criminal violations. In the wake of several serious recent ethical and criminal investigations into the pharmaceutical industry in recent years – companies such as GSK take this duty extremely seriously. As part of this effort – they hired people like the man I am interviewing today. Mr. X is surprisingly charming, amiable, and witty. Somehow as a ‘trigger man’ for a big company, and former NYC police officer, the gentleness, and the compassion emanating from him is unexpected. He tells me that he has received thank you letters from people who were ‘separated from the company’ on his say-so – and I am not surprised.
We talk about public and health care providers perceptions of the pharmaceutical industry, and trends of the past. We discuss the previous ‘bribe and gift’ atmosphere of the past – and he gently calls me out for my Pfizer bag from a long-ago conference. [Ironically, I’ve railed against this bag in the past – it’s from a conference I attended as a student, but hypocrite that I am – have neglected to throw it out. In my own weak defense – I will say that I never again have accepted or received ‘sponsored’ gifts or items.] But he’s right – and I accept my scolding, hopefully with the grace it was given.
He talks about one of the new projects that GSK is implementing – and I immediately sit up and take notice. Phasing out the ‘hootie girls’ as we call the often scantily clad, inappropriately dressed, invariable young, attractive (and always! well-endowed) pharmaceutical representatives that cold call doctors offices with girlish laughs, lots of legs and sample supplies of costly drugs. No, I will not be sad to see the end of the ‘hootie girls’.
Replacing the hootie girls will be nurse educators. Instead of pushing costly brand name drugs – they will be restricted from mentioning brand specific medications.. But educate they will. Hopefully these educators will serve as a resource for healthcare providers – to assist us and inform us without trying influence us. In many ways – it sounds like GSK may be moving in the direction that we need to go.. Afterall – with millions of millions of people needing treatment (and the vast amount of disease out there) just obtaining and supplying these patients with the medications they need is a phenomenal effort – and companies can still make a HUGE profit on volume alone. (And I am not against making a profit – it supports drug research etc..)
But the idea of being able to use the vast amount of information collected from these companies and their volumes of research without rancor, or hardcore skepticism – is encouraging. If we can build bridges and trust – we can ultimately better serve our patients.. Of course, nothing this big ever goes off without a hitch, and Rome wasn’t build in a day – but it’s a start..
It’s a hopeful view from an unlikely source at the end of a very long day that started in one country and ends in another..
* I didn’t get a chance to ask his permission to write about our meeting – so in fairness, I have omitted his name.
The STACCATO trial of TAVI (percutaneous aortic valve implantation) was halted due to problems, and the new data from the PARTNER A trial is less optimistic than previously hoped. More information from two articles published at the Heart.org (Heartwire.com) are re-posted below:
STACCATO: Transapical TAVI in surgery-eligible patients stopped due to adverse events
Nov 10, 2011 Michael O’Riordan
San Francisco, CA– A study comparing the transapical approach for transcatheter aortic-valve implantation (TAVI) against conventional aortic-valve replacement surgery was stopped early due to an increase in adverse events, including an increased risk of major stroke and severe paravalvular leakage, in elderly patients eligible for surgery.
Dr Leif Thuesen (Aarhus University Hospital, Denmark), who presented the results of the STACCATO trial today at TCT 2011, said he is concerned about extending the indication of transapical TAVI to include patients who are candidates for surgery, especially given the increased risk of major stroke observed in this trial.
“There is no doubt there are patients who can’t be operated on, and they should be treated with TAVI,” Thuesen told heartwire. “But the patient who can be operated on—here, we should be very, very cautious. It’s the operable patients, the low-risk patients; they should not have the TAVI procedures, but that’s what is happening. We had one patient, for instance, who did not want the conventional operation, so he had the TAVI procedure in Canada. That’s how it is. Indications are slipping.”
The results of the study were presented during the late-breaking clinical-trials session, as well as during a morning press conference. After Thuesen’s presentation to the media, Dr Michael Mack (University of Texas, Dallas) pulled no punches in his criticism of the trial, saying the study was poorly designed and poorly executed. Mack said the trial was designed too optimistically and powered for event rates in the TAVI arm that were too low. Moreover, some of the events that stopped the trial, including one patient in the transapical-TAVI arm who died while on the waiting list for the procedure, skewed the results.
“I think there is some misinformation here, based on invalid trial design, that is likely to hurt the field,” Mack told heartwire.
The STACCATO trial
The STACCATO trial was designed three years ago and included elderly patients with valvular aortic stenosis who could be treated with surgery or transapical TAVI. Based on data from a surgery registry, they anticipated a surgical-event rate—defined as a composite of 30-day all-cause mortality, major stroke, and/or renal failure—of 13.5% and an estimated event rate in the TAVI arm of 2.5%. The study was stopped due to an increase in adverse events in the TAVI arm after the inclusion of 70 patients.
Indications are slipping.
Regarding the primary end point in the transapical-TAVI arm, there was one non-treatment-related death, one left coronary artery blockage, two major strokes, and one patient who had renal failure requiring dialysis. In the surgical arm, there was one case of perioperative major stroke. Other adverse events in the TAVI arm included a transient ischemic attack followed later with a major stroke, two perioperative cases of severe paravalvular leakage, one perioperative aortic rupture, one left main occlusion during balloon valvuloplasty, and one case of major bleeding.
Thuesen emphasized that the study was initiated three years ago and that the transapical TAVI devices at that time were relatively “unsophisticated” and not available in the full range of sizes now on the market. Moreover, he noted that the study investigators were optimistic about the success of TAVI in this population, especially given their absence of clinical events before the study was started, and for that reason they assumed an event rate of 2.5%, which he admitted was “completely wrong.” He noted that the trial began after investigators had performed approximately 40 transapical TAVI procedures.
To heartwire, however, Mack said the event rates were too low and that investigators should have estimated an event rate closer to 13%, similar to the event rate assumed in the surgical arm. Dr Joseph Bavaria (University of Pennsylvania, Philadelphia), on the other hand, saw a silver lining in the data, especially for surgeons. He said that the study shows the great surgical results obtained in patients with an average Society of Thoracic Surgeons (STS) risk score of 3.4.
Discussing the results and the stopping of the trial, Thuesen said that operators are now much better at handling paravalvular leakage, and newer devices might provide a much better fit into the aorta. Moreover, multislice computed tomography (MSCT) is able to provide better preoperative assessments over echocardiography, which was used in STACCATO. Still, despite the limitations of the trial, Thuesen said that in the current phase of development, transapical TAVI is likely inferior to surgery.
Asked about patients who want TAVI despite eligibility for surgery, Thuesen told heartwire that “we should try to persuade them to have surgery, no doubt.” Mack, on the other hand, said that on the front lines surgeons are forced to tell patients that their surgical risks are too low for TAVI and that surgery is the recommended treatment. “The patients don’t want what I’m selling,” said Mack.
[I completely disagree – of course patients want what Dr. Mack is selling – a quick, easy fix.. Who is he kidding?? That’s why it’s important that we make sure the procedure is safe before expanding the indications for TAVI. – Cartagena Surgery].
In a second article published in the last 24 hours over at Heartwire, results from the PARTNER A trial are also less optimistic than expected.
PARTNER QoL data hint transapical TAVI falls short of aortic-valve surgery
Nov 10, 2011 Shelley Wood
San Francisco – Quality-of-life (QoL) data from the PARTNER A trial should prompt a “rethink” of how many transcatheter aortic-valve implantations (TAVI) are performed via the transapical route, investigators say.
New QoL data released today at TCT 2011 show that while high-risk, surgery-eligible patients treated via a transfemoral route in PARTNER A reported substantial QoL benefits compared with surgery in the early weeks postprocedure, this was not the case for patients treated via a transapical route.
In fact, said Dr David Cohen (Saint Luke’s Mid America Heart Institute, Kansas City, MO), who presented the results, “for patients eligible only for the transapical approach, there was no benefit of transcatheter aortic-valve replacement over surgical aortic-valve replacement at any time point, and in fact, QoL tended to be better with surgical replacement both at one and six months.”
Life after TAVI
As previously reported by heartwire, PARTNER A tested the Edwards Sapien valve against surgery in high-risk patients, with all suitable patients randomized to TAVI undergoing a transfemoral procedure if appropriate and a transapical procedure if the patient was deemed unsuitable for a transfemoral approach. At one year, the transcatheter procedures were found to be noninferior to surgical replacement for the primary end point of one-year mortality.
For a number of secondary end points, TAVI and surgery were associated with differences in procedure-related complications and valve performance at 12 months, but the impact of these differences on patient QoL was previously unknown, Cohen said.
For the current analysis, Cohen et al measured QoL in PARTNER A using the Kansas City Cardiomyopathy Questionnaire (KCCQ), the SF-12, and the EQ-5D, with questionnaires administered at one, six, and 12 months.
For the overall comparison, researchers saw differences between TAVI and surgery at three months, but these had disappeared by six and 12 months. What was clear, however, was that there was significant interaction between the treatment effect and the type of TAVI procedure.
Cohen and colleagues therefore conducted further analyses of QoL according to whether patients had undergone a transfemoral or transapical procedure.
QoL improvements
“For the transfemoral group, the message is one that clinicians won’t find surprising,” Cohen said—these largely reflect the QoL findings from PARTNER B. The less invasive nature of the transfemoral [TAVI] procedure results in pretty important differences in QoL at one month, although by six and 12 months the patients have really come together.”
At one month, however, the improvement in QoL was meaningful—in line with about a one to 1.5 level improvement in NYHA class, Cohen said.
“But on the flip side, the transapical group was really somewhat of a surprise and showed certainly no benefit in terms of QoL of transapical over surgery at any time point, not a hint of a benefit. And for several different measures, [transapical TAVI] was actually doing worse. The trends were all toward worse QoL at one month with the transapical approach.”
At one month, scores were numerically lower for transapical TAVI compared with surgery across the various QoL scales used. At six months, this difference was actually “of borderline statistical significance” at p=0.04 for the primary end point (KCCQ overall summary). By 12 months, all differences disappeared.
The hardest cuts
His hypothesis, although it’s yet to be proven in this setting, is that healing from the medial sternotomy is actually easier and less painful than healing from the smaller, cosmetically “better” lateral thoracotomy used for transapical TAVI.
“A lot of what really hurts and impairs breathing and other sorts of things in these patients after cardiac surgery is motion of the wound. So if the wound is fixed, if the sternum is wired back together so it really can’t move, patients heal quite well, and it doesn’t cause a tremendous amount of pain once the first couple days are past. Whereas the smaller incision, the lateral thoracotomy, is always moving every time you take a breath. There is no way to wire that back together. I think it’s a more painful incision for patients to recover from.”
Cohen expects his presentation to meet with much debate, since it’s the first real suggestion that TAVI is not better than surgery, at least via the transapical route.
Indeed, in a morning press conference, surgeons Dr Michael Mack (Baylor Health Care System, TX) and Dr Joseph Bavaria (University of Pennsylvania, Philadelphia) both made the point that many of the US PARTNER centers actually performed very few procedures over the course of the trial, such that the transapical results truly represent a very early experience with this procedure. To heartwire, Bavaria noted that some of these transapical patients actually had complications that kept them in the hospital longer than expected. “I’d like to see the data from the continued-access registry, to see if those patients did better,” Bavaria said.
And Cohen agreed that centers in Europe, which have a longer history with these devices and procedures, may have found ways of improving patient recovery, involving better technique or using local anesthesia or nerve blocks, after transapical TAVI.
Already, however, while some registry data in Europe have pointed to much better results with a TA approach than those reported today, other European data have hinted that alternatives to the transfemoral route, such as the subclavian approach, may yield outcomes closer to those of the transfemoral route. So far, the Medtronic CoreValve is the only established TAVI device (approved in Europe) that can be implanted via a subclavian route. The CoreValve is still in the early stage of its pivotal clinical trial in the US.
Cohen acknowledged that done well, the transapical procedure is “slick, smooth, and quick,” but “we can’t assume just because the incision is small that the procedure is going to be easier to recover from.”
Asked what he thought the future of the transapical approach might be, Cohen replied: “I think it’s going to have a role, but I’m hopeful that this analysis leads us to reconsider the extent of that role. And for places that have access to multiple technologies for doing nontransfemoral procedures, this should be taken into account. And we may want to really rethink how much transapical we do.”
Mack, however, was less concerned, pointing out that the surgery group in PARTNER A did better than expected. “I think we cannot ignore [these results] and say there are not some concerns here . . . but I’m not as concerned about it as the data may [suggest].”
Still, the results should raise some eyebrows, experts speaking to the media seemed to agree. Dr Samir Kapadia (Cleveland Clinic, OH), speaking at the press conference, said, “This is a little bit shocking. This is a learning [moment]—it’s clear we have to improve the transapical procedure.”
Cohen disclosed receiving grant support/research contracts from Abbott Vascular, Boston Scientific, Medtronic, AstraZeneca, and Edwards Lifesciences and consulting/honoraria/speaker’s bureau fees from Daiichi-Sankyo/Eli Lilly, and Medtronic.
Both of these studies were presented at the 2011 TCT (Transcatheter Cardiovascular Therapeutics) conference in San Francisco – going on November 7th through 11th.
What does this mean for Transcatheter therapies such as TAVI? It means we still have a LONG way to go before we can even begin to consider TAVI as a safe alternative to aortic surgery. The key phrases of concern are ‘indications are slipping’ which means that everything that we’ve suspected/ feared is already occuring – patients are getting TAVI when they should have surgery – (presumably because it’s considered faster/ easier) and less resky – when as readers know: nothing could be further from the truth.
Here at Cartagena Surgery – we embrace technology, but only when it’s used appropriately.
Note: Both of these studies have been re-posted verbatim – with no alterations in written content for the benefit of non-subscribers of cardiology publications. [Comments with article text are clearly delineated as my own, in brackets and italics: Cartagena Surgery].
The FDA recently approved the first TAVI device for aortic stenosis. Currently the device is only eligible for patients who are unable to withstand surgery. But who will end up making that determination? The cardiologist who will be implanting the device? At present – the company manufacturing the Sapien aortic device isrecommending that patients be evaluated by a heart surgeon – but if this follows the typical course, I am sure that this recommendation will be abandoned as a matter of course.
Hopefully, the industry (interventional cardiology) will proceed cautiously, after being ‘omce bitten, twice shy” in light of the epidemic overstenting catastrophies.
Here’s the latest news on TAVI in the United States – and the status of the procedure, which is currently undergoing further evaluation by the FDA.
Here are some highlights from the article:
“In July, the FDA’s Circulatory System Device Panel favored TAVI approval in the U.S. The panel voted on three items, including: safety, effectiveness and whether the benefits outweigh the risks. If the FDA accepts panel recommendations, TAVI procedures would be available to U.S. patients.
However, CMS noted that it is aware of the high stroke and death rates associated with TAVI, and said that it remains concerned about adverse events that may occur, particularly when the procedure is performed by less experienced operators. Rates of stroke and death at 30 days were 6.7 percent and 5 percent, respectively, for those who received TAVI. At one year, these rates were 10.6 percent and 30.7 percent, CMS reported.”
As readers know; here at Cartagena Surgery – we’ve advised caution for the time being – until we have more long-term outcome data on transcatheter aortic valves.
However, after much consideration, and discussion with other people both in and outside the field of cardiac surgery – I have decided that I will begin interviewing and bringing more information about the procedure and providers performing this procedure in the USA. Ultimately, while I may personally, (and professionally) feel that the TAVI procedure has not undergoing sufficient rigorous testing for my patients – I do not want to withhold information from them.
So, I have started writing and contacting providers to obtain more information about the physicians and medical centers performing this procedure. I will discuss these providers further in future posts.
The American Journal of Cardiology just published a new meta-analysis (a study looking at a collection of other studies) that evaluates the effectiveness of bariatric surgery for cardiovascular risk reduction. As we’ve discussed before, meta-analyses are often used to sort through large numbers of studies to look for trends and weed out aberrant results or poorly designed studies. (This is particularly helpful when a poorly designed study gives conflicting results in comparison to the rest of the existing studies.) So, we are going to talk a bit more about the meta-analysis.
In this case, the authors started with 637 studies to evaluate, but ended up using the data from only 52 studies involving almost 17,000 patients. The first step of a meta-analysis is to find every single study even remotely related to your topic. So the authors pulled out, printed and looked at every single study they could find talking about bariatric surgery.
Then the authors start eliminating studies that aren’t relevant to their topic because once you take a closer look; a lot of the studies initially gathered aren’t really related to your topic at all. (For example: If the authors gathered all studies talking about Bariatric surgery outcomes – on closer examination – a study about the rate of depression in bariatric surgery patients wouldn’t have any information usable to evaluate cardiac risk in these patients.) Otherwise it would be like comparing apples to oranges.
Once authors have narrowed the pool to studies that are only looking at relevant topics, with measurable results – the authors then examine the studies themselves. The authors evaluate all aspects of the studies: what is the study design, what does it measure, (is it designed to measure what it is supposed to measure?), what are the results? (were the results calculated correctly?) what are the conclusions? what are the limitations of the study?
Then the authors summarize all of the findings, and draw conclusions based on the results. (if 50 studies involving 16,900 people show one thing – and 2 studies involving 100 people show something completely different – the authors will discuss that.)
The strengths of meta-analyses are that they summarize all of the existing studies out there – and provide readers with fairly powerful results because they involve large numbers of people.
For researchers, meta-analyses are cheap – particularly in comparison to designing, conducting a large-scale study with hundreds or thousands of subjects. A meta-analysis doesn’t require federal grants or institutional permissions. It just requires a computer and journal access (along with a good knowledge of study design, statistics).
As you can imagine, the downside of meta-analyses is that they don’t generate NEW knowledge, since they are summaries of other studies. Meta-analyses are also limited by the AMOUNT of data already published. If few researchers have written about a topic, then a meta-analysis isn’t very effective or powerful. (A meta-analysis on three studies involving only 25 total patients, for example).
Now that we’ve discussed the purpose and function of the meta-analysis, let’s discuss the results of Heneghan’s reported results.
Now, readers need to be very careful when reading blogs, and other articles like mine reporting results such as this – because this is filtered, third-hand information by the time it’s published on blogs, or newspaper articles. (First source is the meta-analysis itself – which as we’ve discussed is actually a summary evaluation of other work). Secondary is the Medscape article which summarizes and discusses the results of Heneghan’s study.
Now, that means that anything you read here is essentially third-hand information – if it’s based on the Medscape article. That’s why we provide links to our sources here at Cartagena Surgery – so readers can read it all first-hand. This is important because just like the children’s game of telephone, as information is passed from source to source, it is edited, filtered and subtly changed (for reasons of space, editorial preference etc.)
heneghan’s meta-analysis results showed significant reductions in weight, blood pressure, cholesterol and hemoglobinA1c (blood glucose levels) after bariatric surgery. The Framingham risk score (a score developed based on the landmark Framingham study) which predicts the risk of cardiovascular events (heart attacks, strokes) also showed a significant reduction (which would be expected if all the risk factors such as hypertension were improved).
Now, a lot of readers might say, “Wait a minute – isn’t this self-evident? If you lose weight – shouldn’t all of these things (glucose, blood pressure, cholesterol) improve?”
Yes .- logical reasoning suggests that they should – but in medicine we require hard data, in addition to logical reasoning (ie. A should lead to B versus a study with ten thouand patients proving A does lead to B.)
We need to be particularly careful when suggesting or assuming causality from treatments (surgery) for conditions. A good example of this is liposuction. Since liposuction involves the removal of subcutaneous fat – and may result a (a small amount) of weight loss – many consumers assumed that this limited weight loss conferred additional health benefits associated with traditional weight loss. Wrong!
Sucking fat out of your behind (liposuction) will not lower your blood pressure, cholesterol, or blood pressure and does not replace the health benefits of weight loss or exercise. I can hear readers snickering now – but that’s because of my phrasing. For years – many people, some health care providers themselves thought that weight loss, any weight loss lead to the above mentioned health benefits, and that included liposuction related weight loss. It took several studies to disprove this. So, in medicine – nothing is obvious – until we prove it is obvious! (Remember: much of what was “obvious” in 1950’s medicine – is now considered absurd.)
One of these days, I may have to eat my words – and when that day comes; I will be happy to do so (and will do it with a 14-point font). But that day is not today.
As reported by Reed Miller over at Heartwire, there are the first results of a very small Canadian study with average follow-up 3.7 years after implantation.. Unfortunately, its way too small of a sample – and mean follow-up falls short of the five-year mark.
But given the rate of implantation in Europe (Germany, in particular) and the fact that these valves are used in younger patients over there – we should have some large (thousands of patients enrolled) studies with five-year data in just a year or two.. One of two well designed studies with a large study population would sure make a lot of us over here (in the USA) feel a lot more comfortable about the safety and efficacy of these devices in our patients.
(I’ll re-post below so you can see for yourself.) I’ve also included links to our little collection of TAVI articles here – or the ‘TAVI library” for first-time readers to catch up.
CoreValve TAVI maintains durability out to four years in small study
(Reed Miller)
[Bold type from original article]
Paris, France – The longest follow-up of patients implanted with the CoreValve (Medtronic) transcatheter aortic-valve implantation (TAVI) device presented so far suggests that it is reliable and durable in high-risk patients, according to the study investigators [1].
“In due time, I’m sure we will see a gradual decrease in the average patient age, treating patients with less comorbidity than was done in the beginning, strengthened by these types of results showing the durability of the implants,” study lead-investigator Dr Peter den Heijer (Amphia Hospital, Breda, the Netherlands) told heartwire.
Here at the European Society of Cardiology 2011 Congress, den Heijer presented long-term follow-up results from 52 patients implanted with the second-generation version of CoreValve in 2005 and 2006 in Europe and Canada. All of the patients in the study were at least 80 years old with a logistic EuroSCORE over 20 or over 65 years old with at least one high-risk comorbidity. All of the patients had severe aortic stenosis and an aortic-valve annulus diameter between 20 mm and 24 mm. Two-thirds of the patients had NYHA class 3 heart failure and almost 20% had class 4 heart failure.
Four-year follow-up data was collected on 20 patients, but 26 patients died, including 13 cardiac deaths. Overall survival was 58.5% at two years and 45.1% at four years. At four years, the surviving patients showed significant improvement in heart-failure symptoms, with 61% in class 1 heart failure and 22% in class 2. Nearly a third of patients showed grade 2 or 3 aortic regurgitation at baseline, but after four years 57% showed no regurgitation and 43% showed grade 1 regurgitation. The mean valve gradient decreased from 41 mm Hg at baseline to 12 mm Hg at 30 days and 10 mm Hg at four years.
There were no strokes reported in the study population between three months and four years and no frame fractures, valve migrations, valve endocarditis, or structural valve deteriorations leading to stenosis or regurgitation. “That’s important, because the goal of this treatment is to provide patients with severe aortic stenosis, a severely life-limiting disease, with a better prognosis, and it appears to be not at all hampered by the structure of the valve,” den Heijer told heartwire.
In a 70-patient study by Dr Ronen Gurvitch (University of British Columbia, Vancouver) colleagues, the Sapien (Edwards Lifesciences) transcatheter aortic valve showed no structural valvular deterioration, stent fracture, deformation, or valve migration over a mean follow-up of 3.7 years [2].
CoreValve is available in Europe and is being tested in a major US clinical trial that Medtronic says will be completed in 2012. The FDA is expected to approve Edward’s Sapien TAVI device soon, following a positive appraisal by its advisory committee.
Still much too early to assess long-term TAVI results
Surgeon Dr Craig Miller (Stanford University, CA), one of the investigators of the pivotal PARTNER trial of Sapien, told heartwire that while the four-year results with CoreValve are “decent,” the clinical community will “need much larger numbers of patients followed at two, three, and four years for the hemodynamics to mean much.”
PARTNER investigator Dr Michael Mack (Medical City Dallas Hospital, TX) told heartwire, “Although it’s reassuring that there are now results out to four years and there’s no sign of structural valve deterioration, it really adds minimal information to what we know already.
“There’s only 20 patients alive at four years, so how do you know what happened to the other 30 patients [in the trial]? Some died of cardiac death and some died of unknown causes. How do you know they didn’t die of structural valve deterioration?” he said. “A better way of doing this study for all aspects is that all the information should be on matched patients.”
Mack said that the real long-term durability of transcatheter valves will become more clear with more data from the SOURCE registry and the long-term follow-up of PARTNER trial, which will include annual core-lab-adjudicated echocardiography follow-up out to five years.
In an email to heartwire,Dr Grayson Wheatley (Arizona Heart Institute, Phoenix) pointed out that although the study had a high percentage of cardiac-related deaths, the arrhythmia-related deaths were a smaller proportion than in some other recent studies. But Mack and Wheatley also pointed out that because there was no echocardiographic core lab in this study, the functional assessments of the valve may not have been always accurate.
Wheatley also pointed out that this study used an older version of the CoreValve, so “this study doesn’t relate too well to real-world use of the CoreValve due to new design changes in the valve system, but it does show that, in general, TAVI procedures can be used in high-risk cardiac patients and that there will be long-term survivors.”
TAVI overseas –
As mentioned above, TAVI has rapidly been implemented in Europe. Latin American medicine has begun to embrace this emerging technology as well. In fact, US physicians are travelling outside the country to perform this procedure on their patients (since it’s not FDA approved.)
From a statement by the University of Miami Medical School – International Medicine Institute: [verbatim]
“New Technology Treats Aortic Heart Valve Disease Without Surgery
More on TAVI: A newly published analysis of the existing/ reported data for peri-operative mortality after transcatheter aortic valve implantation looking at 12 previous studies was recently (June) published in the journal of Interventional Cardiology. (While the study looks at the causes of death – we here at Cartagena Surgery – are going to talk about the rate of death in this study.)
Article information:
Causes of Peri-Operative Mortality After Transcatheter Aortic Valve Implantation: A Pooled Analysis of 12 Studies and 1,223 Patients. The Journal of Invasive Cardiology 2011;23(5):180-184.
Raul Moreno, MD; Luis Calvo, MD; Pablo Salinas, MD; David Dobarro, MD; Jimenez Valero Santiago, MD; Angel Sanchez-Recalde, MD; Guillermo Galeote, MD; Luis Riera, MD; Isidro Moreno-Gomez, MD; Jose Mesa, MD; Ignacio Plaza, MD; Jose Lopez-Sendon, MD
Abstract re-posted below.
Background. In order to improve technique and to prevent serious procedural complications during transcatheter aortic valve implantation (TAVI), it is crucial to identify the causes of death of patients undergoing this procedure. Objective. The objective of this study was to identify the causes of death during the procedure and at 1 month in patients with severe aortic stenosis undergoing TAVI.
Methods. 12 published studies with information about the causes of death in patients undergoing TAVI were selected. Overall, 1,223 patients were included in these studies, and 249 deaths were reported (119 at 1 month and 130 at > 1 month post-procedure).
Mortality during the procedure and at 1 month was 2.3% and 9.7%, respectively. The proportion of cardiac deaths was higher at < 1 month in comparison with > 1 month (56% versus 34%, respectively; p = 0.001). At 1 month, the most frequent causes of death were cardiac failure/multi-organ failure (24%), sudden death/cardiac arrest (17%), vascular and bleeding complications (17%), stroke (11%), sepsis (11%), and cardiac tamponade (10%). During the procedure, the most frequent causes of death were cardiac tamponade (39%), cardiac failure (21%), cardiac arrest (18%), and vascular and/or bleeding complications (18%).
In patients treated with the CoreValve system (Medtronic, Minneapolis, Minnesota) versus those treated with Edwards valves (Cribier-Edwards, Edwards-SAPIEN or SAPIEN XT valve, Edward Lifesciences, Irvine, California), deaths at 1 month due to vascular and bleeding complications were less frequent (3% versus 22%, respectively; p = 0.019), but those due to cardiac tamponade (26% versus 6%, respectively; p = 0.019), and because of aortic regurgitation (10% versus 0%, respectively; p = 0.03) were more frequent.
Conclusion. In this pooled analysis, mortality at 1 month after TAVI was 9.7%. The causes of death were widely variable, and of both cardiac and non-cardiac origin. There were some important differences between both devices in the cause of mortality.
How does this compare with conventional aortic valve replacement surgery (AVR)?
In cardiac surgery – surgeons use database calculators. The most popular one is called the STS risk calculator to determine or estimate the surgical risk for specific patients. This calculator is based on thousands and thousands of patients over decades of research to give approximate surgical risk of morbidity (post-operative complications) and mortality by looking at the planned procedure as well as patient risk factors (age, poor heart function, co-morbidities). Other calculators include a European calculator called EUROscore, and a score used by the VA (veteran’s hospitals.)
Well, how accurate are these calculators?
Interestingly enough – at the same time as the TAVI article, an article (Basreon et. al) discussing and comparing each of these calculators to actual results was published in the June 23 issue of the Annals of Thoracic Surgery. (I’ve re-posted the abstract below.)
In their research – Basreon et. al. found the overall peri-operative mortality for aortic valve replacement surgery to be 5.9% which is well under the 9.7% reported in the article by Moreno, et. al (re-posted above) for TAVI.
While the argument can be made that the higher than expected peri-operative mortality in the TAVI group may be secondary to other factors (patient condition at time of TAVI) without more information on patient demographics – it is hard to know.
I, for one, would like to know the average ages of patients in both groups – was the TAVI group made up of non-surgical fragile, 95 year-olds? What specific factors raised their EUROscores? Was it overall heart function, or was it a specific co-morbidity?
It’s difficult to know since it’s a composite of other research data from multiple studies (and since TAVI is widely used in Europe, accounting for as many as 40% of all aortic procedures in Germany, for example) – this data may also reflect many of these patients (who are not frail elderly, for example.)
Reading through the Moreno study – there is little discussion of the actual patient population, except for one small paragraph (re-posted below). Both of these limitations are probably due to the nature of the study – where investigators were pooling the results of several different studies – which is a good strategy to get a wide overview. However, this can make it impossible to go back and look at questions like ours, particularly if the investigators on the original, smaller studies didn’t record / report this information.
[my comments in brackets/ italics]. I have placed data within the article in bold or italics.
“In this study, pooling the results of 12 series, mortality at 1 month in patients treated with TAVI was 9.7%, and mortality during the procedure was 2.3%. These data compare favorably with the predicted surgical mortality, since EuroSCOREs ranged from 12–28%. [this is the risk calculator that Basreon et. al found that grossly overestimated risk in the study re-posted below.]
In the randomized PARTNER trial, a significant reduction (~20% absolute risk reduction) in the 1-year mortality was obtained for patients with severe aortic stenosis and considered not suitable for surgery due to a very high surgical risk when treated with TAVI in comparison with medical treatment. [as you know from previous discussions – medical treatment is exceedingly ineffective for this condition. It would be more helpful if authors had better defined their ‘very high’ risk patient group since multiple studies show that cardiologists, etc. overestimate patient’s surgical risk.]
Importantly, mortality significantly reduced through the years, from 2004 to 2010, probably reflecting not only the learning curve and the technical improvements, but also a better patient selection process. [meaning patients that are ineligible for surgery may also be ineligible for TAVI in some cases.] This reduction in mortality over time has also been observed in single-center experiences.“
Although not statistically significant, mortality at 30 days was higher in patients treated by transapical approach in comparison with transfemoral approach. Probably, the worse clinical profile of patients undergoing transapical TAVI justifies, at least in part, these findings.[7,12]
Ann Thorac Surg. 2011 Jun 23. [Epub ahead of print] Comparison of Risk Scores to Estimate Perioperative Mortality in Aortic Valve Replacement Surgery.
Division of Cardiology, Veterans Administration Medical Center and University of Minnesota, Minneapolis, Minnesota.
Abstract (bolding/ italics from original article)
BACKGROUND:
Transaortic valve implantation has recently been introduced as an alternative to aortic valve replacement (AVR) for high-risk patients with aortic stenosis. However, accurate assessment of surgical risk is critical for appropriate patient selection. We compared the accuracy of The Society of Thoracic Surgeons (STS) risk score, the European System for Cardiac Risk Evaluation (EuroSCORE), and the Veterans Administration (VA) risk score in predicting perioperativemortality after AVR.
METHODS:
We included 537 consecutive patients who underwent AVR for severe aortic stenosis at the Minneapolis VA Medical Center between 1997 and 2008. Observed and predicted perioperative (30-day) mortality rates were compared. Hosmer-Lemeshow goodness-of-fit test and receiver operating characteristic curves were performed to assess the performance of the scores.
RESULTS:
Perioperativemortality rate was 5.9% (n = 32). Predicted mortality rates for the EuroSCORE, STS score, and VA score were 15.6%, 3.6%, and 6.7%, respectively (p = 0.001). The EuroSCORE overestimated mortality in all patients, most notably among those with ejection fraction less than 35% (49% predicted versus 9% observed). The EuroSCORE had poor calibration (goodness-of-fit test p < 0.008), whereas the STS and the VA scores were well calibrated. However, all three scores displayed good discrimination characteristics per the areas under the receiver operating characteristic curves: STS score 0.73 (95% confidence interval: 0.69 to 0.77); VA score 0.66 (95% confidence interval: 0.62 to 0.70); and EuroSCORE 0.68 (95% confidence interval: 0.64 to 0.72; p > 0.05).
CONCLUSIONS:
The EuroSCORE substantially overestimatesperioperativemortality risk in AVR, particularly in patients with low ejection fraction. These data have implications when deciding the appropriate intervention (transaortic valve implantation versus AVR) for high-risk aortic stenosis patients.
In general – the majority of the literature cites peri-operative mortality for AVR at 2.0 – 5.0% (but this is an average of ALL patients, making the calculators our best estimate of predicted risk.)
So what does this mean?
Clearly, when the data from Moreno et. al shows a thirty-day (peri-operative) mortality of almost 1 in 10 patients – it’s a signal we need to proceed with caution, and continue to follow the research.
1. Since the authors report many of these patients at very high surgical risk (presumably due to cardiac status as well as co-morbidities) and 2. we know that in most people aortic stenosis progresses slowly – it stands to reason that we need to consider intervening earlier in the course of the disease. (Before the heart is significantly weakened).
For people with Aortic Stenosis – I’d want to get second/ third opinions from a cardiac surgeon before proceeding with any catheter based valve procedures. I’d bring all of my information, and studies (echocardiogram results, lab results, medication lists) to have a serious talk to the surgeon about my surgical risk – (and ask him to calculate and show my risk based on the STS calculator). I certainly wouldn’t let anyone make any decisions about my health/ care based on my age alone. [we’ve talked about a ‘good 80’ versus a ‘bad 80’ or even a ‘bad 50’ before.]
Then, I would weigh all of the information – and do my best to make an informed decision.
Here’s some follow-up information on the current recommendations / guidelines from the ACC (cardiologists) and STS (cardiac surgeons) on the use of TAVI or catheter-based therapies for the treatment of valvular disease.
Read it for yourself and let me know what you think, but I find it to be a nice, concisely worded document that clearly delineates and spells out the current role of TAVI therapies as a limited therapy for specific populations – at least until we have long-term outcome data. (We can look to Europe and observe their outcomes, in part).
Let’s hope that all the interventionists keep to the fundamental principles outlined here, as part of our commitment to patient care, safety and well-being.
Re-posted from Cardiosource.com
Title:
Transcatheter Valve Therapy: A Professional Society Overview From the American College of Cardiology Foundation and the Society of Thoracic Surgeons
The following are 10 points to remember about this expert consensus document on transcatheter valve therapy:
1. Transcatheter valve therapy is a transformational technology with the potential to significantly impact the clinical management of patients with valvular heart disease.
2. Although the initial experience is positive, evidence exists from only one randomized clinical trial in patients with aortic stenosis and one in patients with mitral insufficiency.
3. Adoption of these techniques to populations beyond those studied in these randomized trials, therefore, is not appropriate at the current time.
4. It will be important to establish regional centers of excellence for heart valve diseases. Criteria for centers performing interventional therapy in valvular and structural heart disease should be established, and the availability of devices and reimbursement for those procedures should be limited to those centers meeting those criteria.
5. The heart team approach should be used with formation of multidisciplinary heart teams within these centers led by primary cardiologists, cardiac surgeons, and interventional cardiologists.
6. Performance of isolated procedures without construction of a dedicated valve therapy program to encompass all aspects of care—including preprocedural assessment in common clinics, joint procedure performance, and common patient care pathways—is not recommended.
7. A national registry of valvular heart disease to perform post-market surveillance, long-term outcome measurement, and comparative effectiveness research should be established. This could be accomplished by linking the ACC’s NCDR® and STS clinical databases to the Social Security Death Master file and Centers for Medicare & Medicaid Services administrative databases in a national ‘research engine.’ This will, in effect, create a national registry of valvular heart disease.
8. Training and credentialing criteria for practitioners in this field need to be developed. Development of criteria for the formation of fellowship programs, as well as postgraduate training with appropriate experience for adequate patient care leading to guidelines for credentialing, is currently underway by multiple professional societies working together.
9. Interpretation of the current evidence by expert consensus documents and appropriate use criteria need to be developed.
10. With society leadership, multidisciplinary partnerships, and cooperation, a reasoned, balanced introduction of this new therapy can be accomplished.
Durham, North Carolina : After a recent visit to the west coast to interview a cardiac surgeon, I am back on the east coast – spending the week down here in Durham to interview the lung transplant surgeons at Duke. I’ll be talking about it over at the thoracic surgery portal in a series of articles.
As we brushed on in a previous article, TAVI (transcutaneous aortic valve intervention) is the newest interventional therapy on the block, per se and is garnering a lot of media and medical attention. One of the biggest concerns from a health care providers’ standpoint – is that we use this therapy appropriately – in the right patients, for maximum benefits.
One of the good side effects of all this media attention is that the undertreatment of aortic stenosis by medical doctors is now being addressed.
Another article – this one from Medpage.com talks about the potential impact of the commercial approval of TAVI in the US. (Currently it has only been used in the United States as an investigational therapy – meaning that fairly strict criteria have been used in patient selection.) Once it’s available commercially, physicians can use it at their own discretion, which is what the American College of Cardiology (ACC) and the Society of Thoracic Surgeons (STS) is attempting to address with these statements. (Like any commercially available product or service, there will be some doctors who will adopt the practice sooner than others and some doctors who will offer it to patients more readily (and even in cases where appropriateness may not have been determined.)
For all of my devoted readers, who have been wondering what I have been doing since I returned from my latest trip to Bogota:
Still traveling around, still interviewing surgeons whenever I get the opportunity. Today, I spent the day in the operating room in Fresno, California watching a very large cardiac surgery case (Aortic valve replacement/ Mitral valve replacement/ Tricuspid Repair (annuloplasty) with multi-vessel bypass) with Dr. Richard Gregory, MD, a native Fresno resident and cardiothoracic surgeon at St. Agnes Medical Center, in a Stanford affiliated surgery program. Today’s case seems to tie in (unplanned) with our previous discussions on valve surgery last week. It was a great – but complex case.
The facility is a private boutique specialty hospital; elegantly appointed with large, well-lit operating rooms. The surgeon was experienced and talented. Most importantly, the patient did beautifully.
All international/ national protocols followed with pre-operative time-out (which consists of several criteria to meet the National Surgical Quality Improvement Project (NSQIP) requirement. (More about this and the surgical apgar scoring system is detailed in Bogota! a hidden gem guide to surgical tourism). Sterility was maintained throughout the case – and the patient’s hemodynamic needs were promptly and properly addressed. Continuous Anesthesia / Perfusion monitoring through out the case.
Surgical Apgar scores not applied (not appropriate for this type of case.)
In other surgery news – this time, plastics and aesthetics – the Food and Drug Administration released a new statement today cautioning consumers on the use of Silicone breast implants. Previously, the FDA had attempted to limit the use of silicone-filled breast prostheses but had been met with significant resistance from groups of consumers who preferred silicone implants over saline filled implants.
In the article (re-posted below) the FDA states that while previous concerns regarding health complications related to the use of silicone implants such as silicone toxicity/ silicone poisoning have not been validated – the FDA cautions that over 20% of women will need to have their breast implants removed within ten years of implantation. This data confirms information provided during previous interviews with plastic surgeons, who stressed that breast implants are NOT a lifetime device, and several surgeons who stated, “Most patients will need the implants changed within ten years.” [notably, during these physician inteviews – the plastic surgeons were not specifically talking about silicone breast implants.]
Article Re-post: Medscape
Long-term complications likely with silicone breast implants
Mark Crane
June 22, 2011 — Silicone gel–filled breast implants are safe and effective when used according to their labeling, but the longer a woman has the implants, the more likely she is to experience complications, the US Food and Drug Administration (FDA) said in a new report released today.
“Breast implants are not lifetime devices,” Jeffrey Shuren, MD, JD, director of the FDA’s Center for Devices and Radiological Health, said during a telephone news conference. “One in 5 patients who received implants for breast augmentation will need them removed within 10 years of implantation. For patients who received implants for breast reconstruction, as many as half will require removal 10 years after implantation.”
Women with silicone breast implants will need to monitor their breasts for the rest of their lives. To screen for silent ruptures, women should undergo magnetic resonance imaging 3 years after implantation, and then every 2 years thereafter, Dr. Shuren said. Women with saline implants do not need regular imaging.
When the FDA allowed silicone breast implants back on the market in November 2006, it required manufacturers to conduct follow-up studies to learn more about the long-term performance and safety of the devices. The FDA’s report is based on preliminary safety data from these studies, as well as other safety information from recent scientific publications and adverse events reported to the agency.
The most frequently observed complications and adverse outcomes are tightening of the area around the implant (capsular contracture), additional surgeries, and implant removal. Other complications include a tear or hole in the outer shell (implant rupture), wrinkling, uneven appearance (asymmetry), scarring, pain, and infection.
Studies to date do not indicate that silicone breast implants cause breast cancer, reproductive problems, or connective tissue disease, such as rheumatoid arthritis, the FDA said. However, no study has been large enough or lasted long enough to completely rule out these and other rare complications.
“Most women report high levels of satisfaction” with their implants, Dr. Shuren said.
The FDA is working with the 2 manufacturers who make silicone breast implants, Allergan and Mentor, to address the challenges in collecting follow-up data on the women who have received these implants.
Approximately 5 to 10 million women worldwide have breast implants. In the United States, 296,203 breast augmentation procedures and 93,083 breast reconstruction procedures were performed last year, according to the American Society of Plastic Surgeons. About half the procedures used saline implants, and half used silicone implants.
Patients with either saline or silicone implants may have a very small risk for a rare cancer called anaplastic large-cell lymphoma (ALCL) adjacent to the implant. However, the risk is “profoundly small,” said Dr. Shuren. “Since 1997, there are only 34 cases in the published literature, and at most 60 cases out of the 5 to 10 million women with implants worldwide,” he said. “We don’t yet know if there is a causal link.”
When the FDA first released information about the risk in January, William Maisel, MD, MPH, chief scientist and deputy director for science in the FDA’s Center for Devices and Radiologic Health, said the evidence suggests that the kind of ALCL found in conjunction with breast implants is less aggressive and is sometimes treatable by simply removing the implant, the capsule, and the collected fluid.
“The FDA will continue to monitor and collect safety and performance information on silicone gel–filled breast implants, but it is important that women with breast implants see their healthcare providers if they experience any symptoms,” Dr. Shuren said. “Women who have enrolled in studies should continue to participate so that we may better understand the long-term performance of these implants and identify any potential problems.”
The FDA is holding an expert advisory panel in the next few months to discuss how postapproval studies on breast implants can be more effective.
The FDA will issue an update at a future date on saline implants, Dr. Maisel said.
All serious adverse effects should be reported to the breast implant manufacturer and Medwatch, the FDA’s safety information and adverse event reporting program, by telephone at 1-800-FDA-1088, by fax at 1-800-FDA-0178, online at https://www.accessdata.fda.gov/scripts/medwatch/medwatch-online.htm, or by mail to MedWatch, FDA, 5600 Fishers Lane, Rockville, Maryland 20852-9787.
I am re-posting an article published in May on the heart.org by Reed Miller regarding the use of Transcutaneous Aortic Valve Intervention (TAVI). TAVI is when a device is implanted in the cardiac cath lab (through an artery) to treat aortic stenosis. Right now, this therapy is still in limited use in the United States, but is used more extensively in Europe where the guidelines are less restrictive.
I was a little disappointed here because I think some of his introductory language shows significant bias – but I think this article certainly adds to some of the discussions we’ve had here at Cartagena Surgery. Even the title reflects a cardiology bias – cardiothoracic surgeons certainly aren’t the only ones who think we should be cautious about the overimplementation of new, experimental technologies in patients who are good candidates for existing (and proven) surgical treatments. I would think that any prudent health care provider, or consumer would be hesitant to wholeheartedly embrace this therapy given the previous and recent cardiology lessons related to both carotid and cardiac stenting.
New technology is great – when it is selectively targeted to specific populations (high-risk surgical candidates such as extreme elderly (90+) or patients with multiple high risk co-morbidities) who would otherwise be ineligible for surgical intervention. But let’s not put our patients at unnecessary risk by selling TAVI as an ‘easy’ fix to people who we know we benefit from aortic valve replacement surgery before we have all the data.
There are still multiple issues to be addressed with transcutaneous valve therapies – we don’t even know the durability of this technology (how long with they last?) or the long-term complications.. Also when we compare ourselves to European practices, we need to remember that ‘acceptable thresholds’ may differ significantly. At what level of risk of stroke are YOU willing to accept? 5 % ? 10% ? 25% ? And doesn’t that depend on whether you are eligible to have other therapies, and what the risks of those therapies are?
Philadelphia, PA – The neurological injury data from the PARTNER cohort A trial of transcatheter aortic-valve intervention (TAVI) underscore the importance of the collaboration between surgeons and interventionalists when making decisions on how to treat patients in need of a new aortic valve, surgeons here at the American Association for Thoracic Surgery (AATS) 2011 Annual Meeting agreed.
As reported by heartwire, Dr Craig Miller (Stanford University, CA) presented new details on the neurological-event data from PARTNER cohort A, which included high-risk patients eligible for either surgery or TAVI. [‘high risk’ needs to be better defined if the patients were considered acceptable surgical candidates.]
The data showed that the risk of neurological adverse events (transient ischemic attack [TIA] and stroke) was slightly higher with TAVI than surgery in the “as-treated” patients, especially in the patients who underwent transapical TAVI because their vessels were too small to accommodate a transfemoral implant, usually because they were obstructed with arteriosclerosis. Rates of major stroke, however, were not statistically different between the two groups in the as-treated analysis. [numbers/ percents – I need hard data..]
Because of the added neurological risk, Miller believes TAVI should not replace surgery for most patients who can withstand surgery. So he is dismayed that it has grown so rapidly in some European countries where TAVI devices are commercially available, even though the durability of these devices has not been proven. “This is not going to be cost-effective, and civilization cannot afford this if they do not last a good amount of time, and a good amount of time would mean something different to a 95-year-old who is inoperable and to somebody under 70 with a very low surgical risk who should have 10- to 20-year life expectancy. So we have to look at valve durability,” he said. [I wholeheartedly agree. All of Dr. Miller’s concerns are valid.]
“There are many [inoperable patients like] the people in PARTNER cohort B, who gained 1.9 quality-adjusted life-years, and it only cost $55K per QALY to achieve that. So for the inoperable cohort, it is cost-effective and actually provides meaningful rehabilitation, but the jury is out for the younger patients,” he said. “But the cost economics of the not-so-sick operable patients is going to be different; they’re still beaucoup sick and old in PARTNER A, but to take this down to younger, healthier patients is a huge question mark in my mind and in the FDA‘s mind, because we already have the gold standard of low-risk, durable, surgical [aortic-valve replacement],” Miller said.
Surgeon/interventionalist collaboration is critical
Miller thinks one reason that TAVI has become “a runaway train” in Europe is that in some countries there, interventionalists are able to decide to implant a transcatheter valve without consulting a surgeon or, in some cases, even having a surgeon on site. “The German FederalMinistry of Health didn’t have the backbone to stand up and legislate appropriate use, so it’s a free-for-all. But that would be wrong, especially since we don’t have durability data,” Miller said. Miller said he learned that about a quarter of aortic-valve replacements in 2010 in Germany were TAVI procedures, but Dr John Mayer (Children’s Hospital Boston, MA) reported at the meeting that the figure is now around 40%.
A good amount of time would mean something different to a 95-year-old who is inoperable and to somebody under 70 with a very low surgical risk who should have 10- to 20-year life expectancy.
Mayer and Dr Grayson Wheatley III (Arizona Heart Institute, Phoenix) echoed Miller’s concerns about overenthusiasm for TAVI during a staged luncheon debate on whether or not expensive technologies like TAVI ought to be somehow rationed to control healthcare costs. Mayer took the position of defending rationing and Wheatley argued against it, but they both agreed that physicians and their professional societies ought to work to ensure appropriate use of TAVI.
Wheatley said, “We’re probably going to see something along the carotid-stent paradigm, where it’s FDA approved, but [the Centers for Medicare & Medicaid Services] CMS has restricted [coverage] of an FDA-approved device, based on the data and economics, to the highest-risk patients. I see a lot of parallels there.”
“The Medicare national coverage decision process is going to undoubtedly come into play,” Mayer agreed. “That’s one way to control it, and that’s probably the biggest weapon in the arsenal.” Mayer said that the CMS is already discussing a future Medicare coverage policy for TAVI with the Society of Thoracic Surgeons (STS).
“But the other way to control it is to take the combined cardiology/cardiothoracic surgery approach to be careful about how this gets rolled out,” he said. The STS and the American College of Cardiology (ACC) are currently working on a joint position paper that will call for TAVI appropriateness guidelines based on the PARTNER results, Mayer pointed out. That paper will likely be published this summer. “That’s an extremely important step, and I think the government will understand and accept a lot of the recommendations in there.”
Meanwhile, the Society for Cardiac Angiography and Interventions (SCAI) will be contributing to the STS/ACC position paper and is also developing an expert consensus document with representatives from the AATS, STS, and ACC that will outline training and facility standards for performing TAVI. That document will be published prior to the TCT 2011 conference, according to SCAI.
“The difference between how this was rolled out in Europe and how the investigators in the PARTNER trial would like to roll it out in the United States is that a heart team with a surgeon and cardiologists—and not just the interventional cardiologists, but general cardiologists—make the decisions jointly. That is the model that we think should be imposed going forward,” Mayer said. This collaboration will “be a way of us fulfilling our professional responsibility and making sure that this gets rolled out with high quality and will have the side benefit of keeping it from going nuts like it has in Europe.”
While some may be better off undergoing surgery than transfemoral TAVI, there are also some patients whose risk of neurological injury is so high due to arteriosclerotic burden that they are probably not suitable for either surgery or TAVI, Miller said. “The only thing that’s going to change that is more rigorous patient selection and just saying no,” Miller told heartwire. “That might not go over well in the US where everybody demands everything yesterday, [but] since these are patient-disease-related predictors, more rigorous patient selection is the only thing that will reduce the late hazard of neuro events [in patients with very high arteriosclerotic burden].”
What does PARTNER cohort A reveal about the cause of strokes?
STS president and PARTNER investigator Dr Michael Mack (Medical City Dallas Hospital, TX) told heartwire, “There was an initial thought for the past few years that the transapical might be more neuroprotective than the transfemoral because you don’t transverse the aortic arch with the device, and I think this puts to bed that that was not the case. In fact, the stroke rate was higher in the transapical than in transfemoral, but the presentation showed that it was clearly related to the patient substrate.” The one-year stroke rate in the transfemoral-eligible surgery patients was 1.9%, while the one-year stroke rate for the same surgical procedure in transfemoral-ineligible patients was 9.7%, Mack pointed out. “That says they’re different patients [with] a higher atherosclerotic burden.”
[Collaboration will make] sure that [TAVI] gets rolled out with high quality and will have the side benefit of keeping it from going nuts like it has in Europe.
Mack pointed out that the version of the Sapien valve (Edwards Lifesciences) tested in PARTNER was a first-generation device that did not have the nose cone that newer versions will have, “so you basically had this snowplow that could go across the aortic arch and scrape stuff off; smaller delivery devices with nose-cone protection may be expected to be of benefit,” Mack said. However, previous studies with transcranial Doppler show that the majority of the emboli come from the valve during balloon valvuloplasty and deployment of the valve and not from the aortic arch. “[This is] why you don’t see a benefit of the transapical here, because you’re still blowing up that valve [inside the native valve].”
This explanation is consistent with the study’s finding that, in the first few weeks following the procedure, a smaller valve opening area, which is usually a sign of high calcification around the opening, was associated with a higher risk of neurological events in the TAVI patients. Embolic-protection devices, such as Edwards’s Embrella, may catch some of these emboli released during the valve deployment, Mack said, but clinical experience with these devices is very limited so far.
Better devices may stop a lot of the periprocedural events, but about half of the neurological events happened after the periprocedural period. In this period, the most important risk factor—other than undergoing TAVI instead of surgery or being transfemoral ineligible—was a stroke or TIA within the previous six to 12 months. Atrial fibrillation, which was predicted by some to possibly be a risk factor for strokes, was not associated with an increased risk of neurological events in the study. Dual antiplatelet therapy was recommended for all patients in the trial, but the trial could not track how compliant patients were with that therapy.
“We have absolutely no clue if these strokes were device related or not. We don’t know if the device is thrombogenic, or if all that calcium left in the aorta hanging out eventually breaks out, or if it’s a nidus for clot formation and that breaks off. We just don’t have any insight on that,” Mack said.
PARTNER was sponsored by Edwards Lifesciences. Miller has consulting arrangements with Medtronic CardioVascular, Abbott Vascular, and MitraClip. Mack consults for Edwards Lifesciences and Medtronic.
An interesting new article on the use of echocardiography (cardiac ultrasound imaging) to determine the optimal timing of aortic valve replacement is re-posted below. This article is helpful for several reasons, but first a quick summary of Aortic Stenosis.
The timing of aortic valve replacement surgery for aortic stenosis (here after referred to as AS) has always been a complicated issue. Not all stenotic valves need to be replaced at the time of diagnosis; in fact, most don’t since AS is usually diagnosed early (from the presence of a new heart sound on physical examination.)
Patients may not need surgery for ten or twenty years after AS is initially detected, and performing surgery at the RIGHT time is important. Performing surgery too early has almost as many drawbacks as performing surgery too late.
Ideally, surgery is performed before the patient becomes symptomatic (fainting/ near fainting, chest pain or the development of heart failure) AND before the development of heart damage from AS.
Article re-post: [my comments in brackets] I have also italicized certain portions for emphasis.
Echo predicts mortality in untreated
Aortic stenosis with normal LV
function
Article authored by Marlene Busko, Heartwire.com (June 17th, 2011)
Montreal, QC – Researchers have identified four echo markers that predicted mortality in elderly patients with severe aortic stenosis but preserved LV function who did not undergo surgical valve replacement [1]. DrEddy Barasch (St Francis Hospital, Roslyn, NY) presented the study here at the American Society of Echocardiography (ASE) 2011 Scientific Sessions.
The four echocardiographic markers that predicted poor survival were greater left ventricle (LV) concentric remodeling, lower stroke volume, elevated LV filling pressures, and mildly elevated pulmonary artery pressure.
“Our findings may not be generalizable, but they suggest that in [elderly, symptomatic patients with untreated aortic stenosis] with normal LV function, no other valve disease, and normal sinus rhythm, these echocardiographic parameters may be useful for risk stratification,”
Barasch told heartwire. Being able to predict mortality with surgery vs medical therapy in patients such as these—who are typical of patients seen in clinical practice—will become even more important when transcatheter aortic-valve implantation (TAVI) becomes available, he added.
The data suggest that “not operating on symptomatic patients like this—with these markers—is really a death sentence,” said Dr Malissa Wood (Massachusetts General Hospital Heart Center, Boston), when asked to comment on the study.”When you are managing patients who may in fact be good candidates for surgery, looking at their echo and figuring out if
they have these risk factors can help determine the patients’ overall risk of
mortality with surgery vs medical therapy,” she added. [I completely agree with Dr. Woods, which is why we need to be frank in our discussions of the real risks of surgery and the risks of NOT having surgery.]
Surgery seen as “too risky”
The prevalence of aortic stenosis increases with age, and it is estimated that among 80-year-olds, as many as one in four have aortic stenosis, and about 3% to 5% have severe aortic stenosis, Barasch explained. However, a significant proportion of patients with aortic stenosis—30% to 40%—are denied surgery for various reasons, he noted. The patients may have
multiple comorbidities, be too old and frail, or may not want to have surgery.
In some cases, a primary-care physician may not refer a patient for surgery due to perceptions that the procedure is too risky, while in others, a surgeon may decide that a referred patient is not a good candidate for surgery, Wood added.
[The wording here is deceptive – if a patient decides not to have surgery – they weren’t ‘denied surgery’. People have the right to decide for themselves – as long as we ensure that we explain everything to them in terms they can understand. This phrasing is concerning now that many cardiologists are performing experimental transcutaneous valve procedures – sounds like cardiologists are opening the door to doing this procedure in patients that may not otherwise be candidates under “the patient was denied surgery/ patient refused surgery” model which we’ve seen many times before with stent patients.]
[The other issue that we will talk about in a future post is the “primary care provider (PCPs)” not referring patients that he/she doesn’t think are good candidates. Frankly, most PCP and cardiologists, for that matter, are not qualified to make that determination. As you will read further into the article and see – the outcomes of untreated AS are quite grim, so the
decision on whether or not to refer a patient for evaluation, is not one to be taken likely.]
“On the other hand, if you don’t treat these patients surgically, mortality is increased twofold,” said Barasch.
Although most elderly patients with severe aortic stenosis have preserved LV function, few studies have examined how risk factors affect survival in this patient subset. To identify echo variables associated with mortality in these patients, the team reviewed the charts of 443
consecutive patients with severe aortic stenosis and preserved LV ejection fraction who had echo Doppler in their center from 2003 to 2010.
After patients who underwent surgical aortic-valve replacement were excluded, the study population comprised 274 patients with a mean age of 79.5 years (51% men). [this is quite a large subset of patients that didn’t/ couldn’t/ didn’t want surgery. I’d like to know why, and who decided (other than the patients themselves). We successfully do aortic valve replacement in many patients over 80 (age itself should NEVER be a factor – as discussed in numerous previous posts.]
All but two patients had symptoms of heart failure (45%), angina (33%), syncope (5%), or multiple or other symptoms (17%). All patients had normal sinus rhythm, and their mean LVEF was 64.5%+9.4%.
After a mean follow-up of 3.2+2.7 years, 50.5% of the patients had died.
The patients who survived were younger, had a higher body-mass index (BMI), and were less likely to have hypertension, renal insufficiency, diabetes, or heart failure, and more likely to have CAD.
Of the multiple echo-Doppler variables that were examined, only four parameters—LV concentric remodeling (increased LV wall thickness), lower stroke volume, elevated LV filling pressures, and mildly increased pulmonary artery pressure—were moderately associated with mortality, after researchers adjusted for age, gender, and BMI.
No surgery also ups risk
“The biggest take-away message is that we are still grossly undertreating symptomatic aortic stenosis, and many patients who would benefit from surgery are not getting it,” Wood summarized. The study helps identify the magnitude of the risk of not having surgery, among these elderly patients. [Actually, we’ve known these statistics for at least twenty years – I had to memorize them for student rounds when I was graduate school, as standard fare for grilling by the cardiac surgeon.]
“It is a strong study—useful for risk/benefit analysis,” she concluded.
Unfortunately, much of this article seems to state that the biggest obstacle to patient care, safety and welfare seems to be the referring physicians themselves. In my opinion, ALL patients with AS should be referred to a cardiac surgeon (not because I work for one) but because ONLY the surgeon and the patient can truly decide whether its’ time for surgery/ and if the benefits outweigh the risks.
So, if you have Aortic stenosis, symptoms or not – get your more recent echocardiogram, a list of all your medications, and as many medical records as you can get – and schedule an appointment with a cardiac surgeon for a second opinion.
I’ll be posting some additional articles and references for interested readers soon.
I apologize, but the best analogy I can use – is a squeeze ketchup bottle.
okay, it's not heinz.. but you get the picture..
In normal valve functioning, the three valve leaflets open and close fully to permit and control the flood of blood from the left ventricle to the aorta, where it is then circulated throughout the body.
normal valve diameter
During diastole (the filling phase) the leaflets are shut to prevent blood from leaking backwards from the aorta into the heart. (When leaflets don’t close properly this is called aortic regurgitation.)
During systole, the ventricle contracts like a big fist, squeezing the ketchup bottle to shoot blood out of the heart into the aorta. (The force of this is measured in millimeters of mercury, and is the top number on your blood pressure cuff). When the valve is working normally, it opens fully and the blood is ejected out to the aorta, and the whole cycle begins again.
In Aortic Stenosis – the valve leaflets have become fused together, either from age or disease.
(Some people are born with only two valve leaflets and this means that they are more likely to develop aortic stenosis as they age.) As aortic stenosis progresses, the opening for blood to pass thru becomes smaller and smaller since the leaflets can not longer open fully, In many people – at the time of surgery – this opening is about the size of the pinhole in the ketchup bottle that squirts ketchup. (The normal sized opening is 2 to 3 centimeters).
average valve opening in severe aortic stenosis
Now, think about how hard a person has to squeeze that ketchup bottle to get some ketchup for hamburgers, fries (and all the other foods I usually scold about in other posts).
In the heart – this pressure is magnified (and can be measured in the cath lab during cardiac catheterization).
As this pressure gets higher and higher to compensate for the narrowed opening, the delicate structures of the heart become damaged, with the heart muscle becoming thicker and less flexible (just like any other muscle with exercise.) Except unlike biceps, a big thick heart muscle is not a good thing, and can lead to heart failure, arrhythmias and sudden cardiac death.
Eventually, as the heart pushes against the increased pressure, over and over (at least sixty times per minute) the heart gets tired from working so hard. As the heart fatigues, it is unable to keep up with demand and patients will begin to develop symptoms.
These symptoms include:
Syncope/ near syncope (fainting or near fainting) as not enough blood is pushed into central circulation and to the brain.
Chest pain – because not enough blood is pushed out to the coronary arteries during diastole. (In a person with aortic stenosis, nitroglycerin can cause problems – as it lowers blood pressure (and force of contraction even further in someone who needs the extra force.)
Heart failure – the weakened and thickened heart can no
longer keep up and blood begins to back up in the left ventricle.
What these symptoms predict:
Once these symptoms develop, doctors can readily estimate the approximate longevity for patients who do not subsequently have surgery.
From the natural history of aortic stenosis (from before we had surgery to treat it) we know that 50% of people with Syncope will die within 5 years.
Fifty percent of people with chest pain die within three years.
And ultimately, fifty percent of people with heart failure die within two years.
These numbers are important, and I want you to remember them for our subsequent discussions on aortic valve replacement because they need to be factored into a patient’s decision whether or not to pursue surgery.