Another case of sketchy plastic surgery reported – this time in Myrtle Beach, South Carolina. Yet again, I would like to caution readers about seeking ‘cheap’ plastic surgery on the internet. (I’m not saying don’t look – please do! But look smartly.) This doesn’t only apply to plastic surgeons, but to all surgeons, physicians, and healthcare professionals.
‘The internet’ is not all the same – the grade of information can vary widely from scientific journals (highly reputable/ reliable) to fiery but heavily opinionated blogs (unreliable/ unscientific) to frankly fraudulent such as in this instance (in the story above). People need to use caution, due diligence and common sense when researching anything, but particularly medical information on the internet. You need to do your homework.
There are a few things to consider when researching medical information/ providers on the internet.
1. Is the information independently verifiable? (and by what sources?)
As a medical writer – this is a huge portion of my job – verifying the information obtained during interviews, etc. But when you are looking to purchase goods or services – you need to do a little investigative work yourself. Luckily, once again – the internet makes this simple.
The first thing you should investigate is – the person making the claims/ and what their focus is. Use this website for an example, if you like. So take the following information (below) – that is easily available on the site..
(If this information isn’t readily available on the site – that should make you suspicious. “Anonymous” blogs or hidden author websites are NOT reputable. People with valid, truthful information have nothing to hide, and are not ashamed to stand by their work/ writings.)
so you’ve gathered the following information from the site:
Author – XXXX credentials claimed/ authority source: Physician (MD/ DO etc.)
Product or service advertised on the site: surgical procedure XX
Use this information to answer the following questions:
1. Who is this person?
2. How do they know this/ what special knowledge do they possess? (for example – a hairdresser shouldn’t be giving medication advice)
3. Can I verify this?
– Medical personnel can be verified thru state licensing boards.
Some states make this easier than others, but ALL states have this information available to consumers. So go to the website of the licensing board (medical board for doctors, nursing board for nurses) and look the person up.
In this example, I am currently licensed in several states – so pick one, and do an internet search for the board of nursing for that state. (Tennessee is particularly easy since they post educational information, license violations etc. on-line). If this licensing information isn’t easy to find on the website, call the board.**
If the website (ie. plastic surgery clinic) lists an address – use that state for your search.
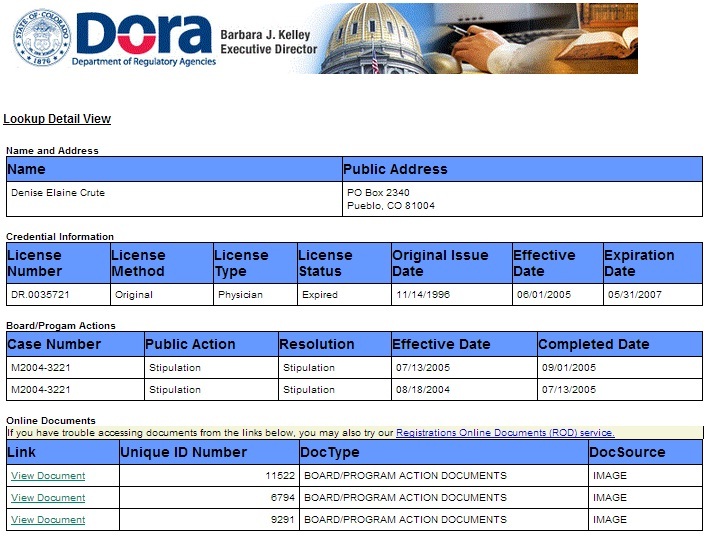
In another example – as seen below – we’ve looked up a surgeon at the Colorado Medical Board.

Looking up a medical license
– All physicians should be licensed in the state of practice (where their clinic is.) If they aren’t licensed in that state – STOP and find another provider. Even if the doctor claims to be from another country, he or she is STILL required to have an active license in the state they are working in.**
Here is an example of physicians sanctioned by the Texas medical board (all of this information is freely available on the internet for your safety.)
Here is another example of a surgeon with multiple medical board actions against her.

license details
Many of the state medical boards will let you read the complaints, actions and disciplinary measures against physicians licensed in that state. However, some states allow physicians under investigation to ‘surrender’ or inactive their license to avoid having disciplinary measures recorded.
– All surgeons, or specialty doctors should also be listed with specialty boards – such as the American College of Surgeons, or the American Society of Plastic Surgery. (While membership is not mandatory, the vast majority of specialty trained surgeons maintain memberships in their specialty organizations.) Other things to consider while investigating credentials:
Do the credentials match the procedure? (Is this the right kind of doctor for this procedure?)
These credentials should match the procedure or treatment you are looking for: such as Plastic surgeons advertising breast augmentation.
This may sound obvious but it isn’t always the case. (for example: dermatologists shouldn’t be doing eyelid lifts or plastic surgery, primary care physicians shouldn’t be giving Botox injections, general surgeons shouldn’t be performing lung surgery etc.)
If you aren’t sure what procedures the doctor should be performing, look at the specialty surgery board – it should list the procedure. i.e plastic surgery and liposuction.
4. After verifying this information, it is time to do a basic internet search on the individual. To do this – perform both a Yahoo! and Google search. This should give you at minimum, 10 to 15 results.
These results should include several non-circular results. “Circular results” are results that return you to the original website, or affiliated websites. For example: Using the information from above – both Google and Yahoo! return several results that link directly to this website. These results also return links for the sister sites. All these of these are circular results – that return you to the starting point without providing any additional outside information.
However, if you scroll down the results: outside links should appear. These should include articles/ publications or scholarly work. Other search results may include more personal information, social networking sites and other newsworthy articles. This gives you a more comprehensive picture of the provider.
One of the things we should mention, is patient testimonials. While many providers include extensive patient testimonials, I disregard these for several reasons:
– There is usually not enough information to verify the authenticity of these patient claims. “I love my doctor. He’s a great surgeon.” – Gina S. doesn’t really tell you anything. In particular, there is no way to verify if there really is a Gina S. or if she is a fictitious creation of the website author. (There have been several cases where people working for the doctors have created ficticious accounts including before and after photos talking about procedures that they never had). Don’t be lulled into a false sense of security with patient testimonials.
– Some people use blogs, or message boards for the same purpose, and the same caveats apply.
– Another reason that patient testimonials are not useful in my opinion, is that patients (and their families) are only able to provide subjective information. Several of the cases in the news recently (of fraudulent individuals posing as doctors) had several “happy patients’ to recommend them. Patients, for the most part – aren’t awake and able to judge whether the surgery proceeded in a safe, appropriate fashion. The testimonials are merely a comment on the physician’s charisma, which may give future patients a false sense of security.
I’ve finished my search – Now what?
Use commonsense:
– Surgical treatments should be performed in an appropriate, sterile environment like a hospital or freestanding clinic. A reputable surgeon does not operate in the back of a motor home, a motel room or an apartment. (All of these have been reported in the media.) If the setting doesn’t seem right – leave. You can also investigate the clinic.
– Bring a friend. In fact, most surgeons will require this, if you are having liposuction or another large procedure. Doctors don’t usually drive their patients around (as was done in several recent cases.) The exception to this rule is medical tourism packages. These packages often include limousine transportation services but these services are provided by a professional driver (not the doctor, or ‘his cousin’). Your friend/ companion is not just your driver – they are also there to help feel out the situation. If something seems amiss – do not proceed.
– if the price is too cheap – be suspicious. If every other provider in the same location charges a thousand dollars – why is this doctor only charging a hundred dollars? Chances are, it’s not a sale – and he/ she is not a doctor.
– Use reputable sources to find providers – Craigslist is not an appropriate referral source.
– Are the claims over-the-top? Is the provider claiming better outcomes, faster healing or an ‘easier fix’ than the competition? (We will talk more about this in a future post on “miracle cures’ and how to evaluate these claims.
I hope these hints provide you with a good start to your search for a qualified, safe, legitimate provider. The majority of health care providers are excellent, however the internet has given criminals and frauds with an easy avenue to lure/ and trap unsuspecting consumers.
** The majority of cases that have been recently reported have taken place in the United States (Nevada, New Jersey, Florida and South Carolina.) Many of the people perpetrating these crimes have posed as Latin American surgeons to capitalize on the international reputation of plastic surgeons from South America. They also used these claims to try and explain away the lack of credentials. A legitimate doctor from Brazil, Argentina, Colombia, Costa Rica or another country, who is practicing in the United States WILL HAVE an American license.
Additional references/ stories on fraudulent surgeons.
(Hopefully this section will not continue to grow)
More on the Myrtle Beach story
Myrtle Beach – a nice article explaining why people should see specialty surgeons
Basement surgery
Article on unlicensed clinics in Asia (medical tourists beware!)
A truly bizarre story about unlicensed dentistry in Oregon
Additional references:
American College of Surgeons – lists doctors distinguished/ recognized as “fellows” in the academic organization, and provides a brief summary of specialties.