For more about my week as a fashion photographer, click here.
I’ll be publishing some more photos over the next week, as I sort through the over 8,000 images I collected during my short stint as a fashion photographer – but the standout collection belonged to the fashion design students at Universidad Pontificia Bolivariana here in Medellin, Colombia.
This slideshow requires JavaScript.
Even the most fantastical designs presented have a plethora of fine detailing and seeming. It is this use of seaming, (and actual sewing techniques) more than fabric choice, use of color or other factors that really makes this collection stand apart from the rest of the runways at Colombia Moda.
It’s in the details..
This attention to detailing also united the different designers and design concepts within the collection – from the plastic ‘raincoat’ jackets, to the corseted black matching his and hers outfits – , the green and white dress princess seamed dress with flared hem and cape sleeves.. The Peter Pan blouse*..
It’s a welcome change from so many designs that rely on cheap accessories or flashy fabrics to carry the look. While these designs certainly benefitted from the lovely (and ethereal – in the case of some of the white outfits) fabrics – the designs could stand without them. Of course, this is the difference between high couture design and mass market items. Mass marketed cheap cotton jersey dresses at Wal-mart (or even the Mall) aren’t going to have this level of detail..
I have some great shots of the models with the designers, which I will add soon. (It’s been a long couple of days – and I can no longer keep my eyes open.
*It’s been over 20 years since I took a few costume studies classes at Dalhousie so some of the exact terminology is hidden in the far recesses of my brain.. But I haven’t forgotten what I like..
Why Colombia is failing to reach its potential as a medical tourism destination
Close proximity to the USA, advanced medical technologies, excellent medical facilities in friendly but cosmopolitan cities such as Bogotá and Medellin make Colombia look like an attractive destination for medical travelers. However, Colombia continues to fail to meet expectations regarding its potential as a preferred destination for medical care. While accurate statistics on medical travel do not exist, patients continue to flock to hospitals in India, Asia and Mexico instead of Colombia.
While I don’t have a degree in business or marketing, after spending over three years investigating and writing about medical tourism in Colombia, much of the problem is readily apparent. Sadly, these problems have nothing to do with medical treatments or patient care which is equal to or superior to that of most North American facilities in the majority of cases. The problem is customer service.
Customer Service is non-existent
The primary problem is a health care model that is essentially devoid of many of the principles of customer service. This is problematic for Colombian citizens but devastating to an industry seeking to recruit customers from overseas. In a study done several years ago, researchers found that if a person is pleased with the service they received, on average, they tell five people. However, if the person receives bad service, they tell 20. In an internet age, make that more like 100, or 1,000 people due to the popularity of message boards and blogs.
How Colombia can become more competitive
But there are several ways that local hospitals could improve their service models and attract more happy clients.
Invest in the industry
While the government of Colombia (Proexport) and many of the facilities themselves have financially invested millions and millions of dollars into attracting medical tourism – there needs to be an equal investment and commitment to service. A good example of this phenomena is at the Fundacion Santa de Bogotá. In the last few years, Fundacion Santa Fe de Bogotá has invested countless financial resources in upgrading their facility, and adopting the John Hopkins brand in a bid to attract more cash-paying overseas patients. Yet, the hospital divested itself of one of its best medical tourism resources, the former head of the International Patient Center, who was the first point of contact for overseas travelers and was known for kindness, competent service and efficiency. In contrast, the new head of the International Patient Center, has established a reputation for not answering emails, and skipping meetings with American visitors. As the first point of contact for many potential consumers, the International Patient Center fails miserably. But this hospital is just one of several in Colombia that are failing to reach their potential due to logistical problems.
How does this happen? There appears to be a communication breakdown between the marketing department and many of the people who should be instrumental in actually attracting and retaining clients.
If it’s not online, it doesn’t exist – and answer your email
As the owner of a large website on medical tourism in Latin America, I receive frequent emails from dissatisfied clients. The number one complaint is a lack of response to attempted email communications. For someone in another country, or who doesn’t speak Spanish, telephone communication is not a reasonable expectation. If the information isn’t on-line, it might as well not exist. Overseas patients are not going to spend innumerable hours searching for specific information about providers and facilities in Colombia when they can find this information quickly and easily on popular search engines for other facilities outside Colombia.
If hospitals don’t reply in a timely fashion, patients will quickly move on to someone who will. Many of the Indian facilities have customer service specialists who respond in 12 hours (or less). In comparison, I recently received several emails from an American in Medellin who had emailed the International Patient Center at the Clinica de Medellin several weeks ago, and still has not received a response.
Copy-edit
When consumers do find English language resources, the information is often rife with spelling errors and multiple inconsistencies. Since this information represents the facility, it gives foreign language visitors a poor impression of what are often otherwise excellent facilities.
Customer service starts at the door
While Colombian security protocols can be daunting in themselves to outsiders, more discouraging is the typical attitudes encountered by visitors after entering the facility. The most notorious of these are the secretaries in many of the doctors’ offices and clinics. While some of these individuals have been pleasant, and welcoming to outsiders, the stereotypical bored yet rude secretary prevails. These nail-filing, eye-rolling employees who often intentionally ignore foreign visitors are a hospital staple in Colombia. Whether avoiding eye-contact while chatting on the phone, or muttering rude comments under their breath; these employees are often a patient’s first impression of medical services in many of the finest facilities in Colombia.
These behaviors along with lengthy waits after the scheduled appointment time, are frequently cited during interviews with international patients.
This isn’t just a lack of courtesy on behalf of lower-level employees, its bad business and it hurts Colombia. These pitfalls shortchange everyone involved in medical tourism; the clients who are turned away (and seek services elsewhere), the doctors seeking to expand their practice, and the hospitals that are losing out on millions of dollars of potential revenue.
Until these problems are addressed, the flocks of patients will continue to travel exorbitant distances to Thailand, India and other destinations that offer better levels of service.
Dr. Juan David Londoño, plastic surgeon (photo provided)
Dr. Juan David Londoño is a plastic surgeon here in Medellin who specializes in body procedures such as liposuction, abdominoplasties and breast augmentation.
He shares an office with Dr. Jorge Aliro Mejia Canas in the Forum building, next to the Santa Fe shopping mall in the upscale Poblado neighborhood.
He is also one of just a handful of surgeons here who specialize in hair restoration.
Dr. Londoño attended medical school at the Universidad de Antioquia, graduating in 1995. He completed his plastic surgery residency at the same institution and completed his training in 2003. While he trained in both reconstructive and aesthesthic plastic surgery, he states that he prefers aesthetic surgery because of the close relationship it entails with patients.
Today we talked primarily about Hair Restoration procedures because it’s his favorite procedure, and one I don’t know much about.
Patience is the key, he states as he explains the ins and outs of hair restoration treatments. Patience was certainly the order of the day as he carefully and graciously explained the principles of hair transplantation to me. Patience is necessary he explains, as in, there is no ‘quick fix’. Hair restoration techniques have evolved with the development of newer procedures but it remains a painstaking process.
Not just for male pattern baldness
While people traditionally think of this treatment as exclusively for male pattern baldness, women also undergo hair restoration in cases of thinning hair. People can also use this treatment to restore hair to other areas of the body such as the eyebrows (or as commonly publicized in Turkey) for beard restoration.
Treatment options
As Dr. Londoño explains, there are a range of treatments available for the treatment of hair loss, such as male pattern baldness, or thinning hair. While these treatments run along a continium of scalp massage –> medications –> surgery; these treatments can also be used to compliment each other.
Probably the best well-known treatments are the medications such as topical applications of minoxidil (Rogaine) or oral (finesteride) Propecia tablets. Many people are familiar with these medications due to long-standing and widely viewed pharmaceutical advertisements in the early and late 1990’s. Both of these medications were originally developed to treat other conditions (hypertension and BPH) and hair growth was quickly noted to be a frequently occurring side effect. These medications underwent additional clinical trials and study by the FDA before being re-formulated (as a topical spray), in the case of minoxidil, and re-marketed to treat hair loss.
However, these medications are less than ideal for treating a long-term problem like hair loss. While the medications can prevent additional hair loss, in most cases – additional hair growth is modest and requires continued medical therapy (pills) to maintain.
Scalp massage, is believed to stimulate blood circulation in the scalp and improve the health of the scalp and hair. It is also quite pleasant for most people. However, the results of scalp massage as a sole treatment are minimal at best when it comes to the treatment of alopecia.
Surgical methods of hair restoration
The original surgical methods of hair transplantation (or hair restoration) are more widely known for their limited results. “Hair plugs” refer to the artificial appearance due to the technique of implanting a group of hair in one area, with the finished results often having a row-like appearance (like a doll).
More modern techniques include the strip method, and the most recent technique called Follicular Unit Extraction (FUE).
With the strip method a small area of scalp on the back of the head (where hair is usually the densest, and has the greatest longevity) is surgically removed in a long strip. The scalp is then sutured closed, leaving a small linear scar. The area of scalp, and hair follicules are then used for implantation. By taking a portion of the scalp, the surgeons are able to ensure that the critical portion of the hair shaft – the root is preserved. This root is needed for hair to survive and grow after implantation.
With the newer Follicular Unit Extraction, each hair, including the root is extracted using a 1mm punch biopsy technique. (This is like a skin biopsy punch but much smaller.) Since each root is extracted individually, this is a painstaking and time consuming process. He reports that depending on the degree of hair loss, the length of the sessions and the results desired by the patient – determines the number of sessions a person will need. Since this procedure requires multiple sessions, some patients elect for shorter sessions but require a higher number of sessions since this is often more convenient for the schedules of working people.
The first treatment is usually done to re-establish the natural hairline. Subsequent treatments are needed to fill in areas of hair loss.
For patients who have very little remaining head hair, hair can be taken from other parts of the body. In general, surgeons use hair from areas (like the so-called “fringe area”) where hair persists despite months or years of hair loss. These areas are less likely to have hair that will succumb to the processes that caused alopecia in these individuals.
There are newer methods of FUE which use a more automated process, but as Dr. Londoño explains this often incurs a higher cost – and does not improve the outcomes (but does shorten the process somewhat.) He has the Artas Robot to assist him with the process, (if needed), but cautions readers not to be fooled by surgeons advertising the latest and greatest machinery. We digress into a conversation about general plastic surgery and the widespread advertising of specifically trademarked (and very expensive) equipment such as SlimLipo, Ultrasound and Vaser.
It’s more about the surgeon than the tools
He cautions consumers not to be fooled into thinking that having the most expensive equipment equals the best surgeon as often these devices are employed only to attract customers and command more expensive prices. As we discussed in a previous post, these devices were designed for specific uses that may not even be needed for many clients.
Why should patients pay for ultrasound-assisted liposuction when standard liposuction will be equally effective in their case? That’s kind of how he feels about the hair transplant robot. He has it – and he will use it if he needs it, but it isn’t for everyone.
Results take time
Results of this procedure are not immediate. The scalp takes time to heal from the transplant procedure, and the newly implanted follicules need to adjust to the transplantation process. Usually, the initially transplanted hair sheds – leaving living, hair producing roots behind. These hair roots will then grow new hair as part of the normal hair growth cycle. But hair takes time to grow – so many patients won’t see the full results of their procedure for up to six months afterwards as the hair grows in to the patient’s normal length.
Costs of the procedure
The near universal standard for hair restoration at many facilities is a dollar a hair. When you consider that the average (full) head of hair contains 100,000 hairs – the potential costs of this procedure* can be daunting. However, Dr. Londoño does not apply a “one price fits all” approach to his patients. Instead his assesses the client, their restoration needs (a small area versus the entire coronal area), the amount (and type) of treatments involved, and the expected results before determining a price. It is a more personalized and individualized accounting that may not suit some medical tourists who are looking for bargain basement prices however, it seems a better practice.
*Generally patients would only need a small fraction of this number for hair restoration.
References and Resources
Khanna M. (2008). Hair transplantation surgery. Indian J Plast Surg. 2008 Oct;41(Suppl):S56-63. An excellent overview of the procedures used in hair transplantation with photographs depicting these techniques and results.
Note: the feature photograph(on the front page) has been heavily edited (by me) to depict a gentleman with a receding hairline. This model actually has a lovely head of hair, but I did not want to use the photo of a real person without permission. (This photo is open source). This photo is for article art only and is not an attempt to dupe or trick readers. It is my policy to always disclose when photos have been altered from the original image.
Security on a street corner in an upscale Bogota neighborhood
Stories from the Front
Anyone want to hear about the summer I spent living with a group of young journalists, in a South American country in the midst of a civil war? Oh, wait – that’s this summer – and it’s not as dramatic as all that. While everything I said in the first sentence is factually correct; it’s also horribly misleading.
I live in an exciting, wealthy cosmopolitan city where the murmurs of FARC and continuing peace talks garner little notice – unless, of course, you are living in the corporate offices of Colombia Reports. But otherwise, paramilitaries are not a big part of my daily life with the exception of the occasional amputee in the park.
(This is not to minimize the horrors faced by the populace for the last fifty years, but to avoid over-sensationalizing daily life here.)
lost his leg due to a landmine
Daily concerns
A bigger concern is a more basic one – for any woman alone in any major city, particularly as a traveler navigating a foreign city, and foreign language: the usual safety concerns to avoid being victimized. So, I worry more about being mugged for my purse than being kidnapped and held by gangs or para-military groups. Living here is like living in Chicago, Detroit, and Washington D.C in that respect. But that’s not always what people want to hear.
Flashy Headlines
Big headlines attract readers, but substance and content are what’s really important. So instead of trading in on ‘war stories’ with my readers, I try to bring portraits of daily life in Colombia and other parts of Latin America. It’s not as flashy; and exciting – but it’s worthwhile reading all the same. So with that in mind, I hope you enjoy reading about the lives of some of the people I encounter in my travels.
Please note that some of the images in this article have been edited to preserve patient privacy.
Today, Dr. Luis Botero has invited me to observe surgery at IQ Interquirofanos in the Poblado section of Medellin. He is performing full-body liposuction and fat grafting of the buttocks.
Dr. Luis Botero, in the operating room
The facility: IQ Interquirofanos
Interquirofanos is located on the second floor
IQ Interquirofanos is an ambulatory surgery center located on the second floor of the Intermedica Building across the street from the Clinica de Medellin (sede Poblado). The close proximity of this clinic to a hospital is an important consideration for patients in case of a medical emergency.
The anesthesiologists estimate that 90% of the procedures performed here are cosmetic surgeries but surgeons also perform gynecology, and some orthopedic procedures at this facility.
The are seven operating rooms that are well-lit, and feature modern and functional equipment including hemodynamic monitoring, anesthesia / ventilatory equipment/ medications. There are crash carts available for the operating rooms and the patient recovery areas.
There are fourteen monitored recovery room beds, while the facility currently plans for expansion. Next door, an additional three floors are being built along with six more operating rooms.
Sterile processing is located within the facility with several large sterilization units. There is also a pharmacy on-site. The pharmacy dispenses prosthetics such as breast implants in addition to medications.
The only breast prosthetics offered at this facility are Mentor (Johnson & Johnson) and Natrelle brand silicone implants (Allergan). In light of the problems with PIP implants in the past – it is important for patients to ensure their implants are FDA approved, like Mentor implants.
In the past seven years, over 31,000 procedures have been performed at Interquirofanos. The nurses tell me that during the week, there are usually 30 to 35 surgeries a day, and around 15 procedures on Saturdays.
Prior to heading to the Operating Room:
Prior to surgery, patients undergo a full consultation with Dr. Botero and further medical evaluation (as needed). Patients are also instructed to avoid aspirin, ibuprofen and all antiplatets (clopidogrel, prasugrel, etc) and anti-coagulants (warfarin, dabigatran, etc.) for several days. Patients should not resume these medications until approved by their surgeon.
Complication Insurance
All patients are required to purchase complication insurance. This insurance costs between 75.00 and 120.00 dollars and covers the cost of any treatment needed (in the first 30 days) for post-operative complications for amounts ranging from 15,000 dollars to 30,000 dollars, depending on the policy. All of his clients who undergo surgery at IQ Interquirofanos are encouraged to buy a policy from Pan American Life de Colombia as part of the policies for patient safety at this facility. International patients may also be interested in purchasing a policy from ISPAS, which covers any visits to an ISPAS-affiliated surgeon in their home country.
Today’s Procedures: Liposuction & Fat Grafting
Liposuction –Liposuction (lipoplasty or lipectomy) accounts for 50% of all plastic surgery procedures. First the surgeon makes several very small slits in the skin. Then a saline – lidocaine solution is infiltrated in to the fat (adipose) tissue that is to removed. This solution serves several purposes – the solution helps emulsify the fat for removal while the lidocaine-epinephrine additives help provide post-operative analgesic and limit intra-operative bleeding. After the solution dwells (sits in the tissue) for ten to twenty minutes, the surgeon can begin the liposuction procedure. For this procedure, instruments are introduced to the area beneath the skin and above the muscle layer.
During this procedure, the surgeon introduces different canulas (long hollow tubes). These tubes are used to break up the adipose tissue and remove the fat using an attached suctioning canister. To break up the fat, the surgeon uses a back and forth motion. During this process – one hand is on the canula. The other hand remains on the patient to guide the canulas and prevent inadvertent injury to the patient.
fat being removed by liposuction
Due to the nature of this procedure, extensive bruising and swelling after this procedure is normal. Swelling may last up to a month. Patients will need to wear support garments (such as a girdle) after this procedure for several weeks.
Types of liposuction:
In recent years, surgeons have developed different techniques and specialized canulas to address specific purposes during surgery.
Standard liposuction canulas come in a variety of lengths and bore sizes (the bore size is the size of the hole at the end of the canister for the suction removal of fat tissue.) Some of these canulas have serrated bores for easier fat removal.
Ultrasound-assisted liposuction uses the canulas to deliver sound waves to help break up fat tissue. These canulas are designed for patients who have had repeated liposuction. This is needed to break up adhesions (scar tissue) that forms after the initial procedure during the healing process.
Laser liposuction is another type of liposuction aimed at specifically improving skin contraction. This is important in older patients or in patients who have excessive loose skin due to recent weight loss or post-pregnancy. However, for very large amounts of loose skin or poor skin tone in areas such as the abdomen, a larger procedure such as abdominoplasty may be needed.
During laser liposuction, a small wire laser is placed inside a canula to deliver a specific amount of heat energy to the area (around 40 degrees centrigrade). The application of heat is believed to stimulate collagen production (for skin tightening). Bleeding is reduced because of the cautery effect of the heat – but post-operative pain is increased due to increased inflammatory effects. There is also a risk of burn trauma during this procedure.
There have been several other liposuction techniques that have gone in and out of fashion, and many of the variations mentioned are often referred to by trademark names such as “Vaser”, “SmartLipo”, “SlimLipo” which can be confusing for people seeking information on these procedures.
Fat Grafting
Fat from liposuction procedure to be used for buttock augmentation
Fat grafting is a procedure used in combination with liposuction. With this procedure, fat that was removed during liposuction is relocated to another area of the body such as the buttocks, hands or face.
In this patient, Dr. Botero injects the fat using a large bore needle deep into the gluteal muscles to prevent a sloppy, or dimpled appearance. Injecting into the muscle tissue also helps to preserve the longevity of the procedure. However, care must be taken to prevent fat embolism*, a rare but potentially fatal complication – where globules of fat enter the bloodstream. To prevent this complication, Dr. Botero carefully confirms the placement of his needle in the muscle tissue before injecting.
Results are immediately appreciable.
fat being injected for buttock augmentation. (Photo edited for patient privacy).
The Surgery:
Patient was appropriately marked prior to the procedure. The patient was correctly prepped, drapped and positioned to prevent injury or infection. Ted hose and sequential stockings were applied to lessen the risk of developing deep vein thrombosis. Pre-operative procedures were performed according to internationally recognized standards.
Sterility was maintained during the case. Dr. Botero appeared knowledgeable and skilled regarding the techniques and procedures performed.
His instrumentadora (First assistant), Liliana Moreno was extremely knowledgeable and able to anticipate Dr. Botero’s needs.
Circulating nurse: Anais Perez maintained accurate and up-to-date intra-operative records during the case. Ms. Perez was readily available to obtain instruments and supplies as needed.
Overall – the team worked well together and communicated effectively before, during and after the case.
Anesthesia was managed by Dr. Julio Arango. He was using an anesthesia technique called “controlled hypotension”. (Since readers have heard me rail about uncontrolled hypotension in the past – I will write another post on this topic soon.)
Controlled Hypotension
However, as the name inplies – controlled hypotension is a tightly regulated process, where blood pressure is lowered to a very specific range. This range is just slightly lower than normal (Systolic BP of around 80) – and the anesthesiologist is in constant attendance. This is very different from cases with profound hypotension which is ignored due to an anesthesia provider being distracted – or completely absent.
With hypotensive anesthesia – blood pressure is maintained with a MAP (or mean) of 50 – 60mmHg with a HR of 50 – 60. This reduces the incidence of bleeding.
However, this technique is not safe for everyone. Only young healthy patients are good candidates for this anesthesia technique. Basically, if you have any stiffening of your arteries due to age (40+), smoking, cholesterol or family history – this technique is NOT for you. People with high blood pressure, any degree of kidney disease, heart disease, peripheral vascular disease or diabetes are not good candidates for this type of anesthesia. People with these kinds of medical conditions do not tolerate even mild hypotension very well, and are at increased risk of serious complications such as renal injury/ failure or cardiovascular complications such as a heart attack or stroke. Particularly since this is an elective procedure – this is something to discuss with your surgeon and anesthesiologist before surgery.
The patient today is young (low 20’s), physically fit, active with no medical conditions so this anesthesia poses little risk during this procedure. Also the surgery itself is fairly short – which is important. Long/ marathon surgeries such as ‘mega-makeovers‘ are not ideal for this type of anesthesia.
Dr. Julio Arango keeps a close eye on his patient
However, Dr. Arango does an excellent job during this procedure, which is performed under general anesthesia. After intubating the patient, he maintained a close eye on vital signs and oxygenation. The patient is hemodynamically stable with no desaturations or hypoxia during the case. Dr. Arango remains alert and attentive during the case, and remains present for the entire surgery. Following surgery, anesthesia was lightened, and the patient was extubated prior to transfer to the recovery room.
He also demonstrated excellent knowledge of international protocols regarding DVT/ Travel risk, WHO safety protocols and intra-operative management.
Surgical apgar score: 9 (however, there is a point lost due to MAP of 50 – 60 as discussed above).
Results of the surgery were cosmetically pleasing.
Post -operative care:
Prior to discharge from the ambulatory care center after recovery from anesthesia the patient (and family) receives discharge instructions from the nurses.
The patient also receives prescriptions for several medications including:
1. Oral antibiotics for a five-day course**. Dr. Botero uses this duration for fat grafting cases only.
2. Non-narcotic analgesia (pain medications).
3. Lyrica ( a gabapentin-like compound) to prevent neuralgias during the healing period.
The patient will wear a support garment for several weeks. She is to call Dr. Botero to report any problems such as unrelieved pain, drainage or fever.
Note: after some surgeries like abdominoplasty, patients also receive DVT prophylaxis with either Arixtra or enoxaparin (Lovenox).
Follow-up appointments:
Dr. Botero will see her for her first follow-up visit in two days (surgery was on a Saturday). He will see twice a week the first week, and then weekly for three weeks (and additionally as needed.)
* Fat embolism is a risk with any liposuction procedure.
**This is contrary to American recommendations as per the National Surgical Care Improvement Project (SCIP) which recommends discontinuation within the first 24 hours to prevent the development of antibiotic resistance.
Dr. Sergio Franco wrote the book on heart surgery.
It was exciting and illuminating to talk to Dr. Sergio Franco, who is one of Colombia’s most prolific writers and professors of cardiac surgery. The 50 year-old cardiac surgeon has authored multiple textbooks for surgeons and edited ten others, making him one of the nation’s definitive experts on cardiac surgery.
Dr. Franco stands near a collection of his textbooks
Currently he is the Medical Director of the Cardiopulmonary and Peripheral Vascular Center of the Fundacion San Vicente in Rio Negro, as well as Chief of Cardiothoracic Surgery at the Clinica de Medellin. For the last 12 years, he has also been the program director for post-graduate studies at the Universidad CES medical school. Between the two clinics, and the five other surgeons he works with (2 at Clinica de Medellin and 2 at Rionegro), he estimates that the cardiac programs see volumes of 700 – 750 cases per year.
For our first interview, we meet at the Clinica de Medellin to talk. He later invites me to see the hospital at Rionegro.
Education/ Training / Experience
Dr. Franco attended medical school, general surgery residency and cardiac surgery fellowship at the Universidad Pontifica Boliviarana. He finished his fellowship in 1996. As part of his fellowship, he spent nine months training in heart and lung transplantation at Loyola University Medical Center in Chicago, Il. During his heart and lung tranplantation training, he received an award as “Best Foreign Medical Fellow.” He graduated with high honors due to his exemplary grade point average.
He has additional training in thoracic and thoracoabdominal aortic surgery (Missouri Baptist, 1998), and minimally invasive valvular surgery (Cleveland Clinic).
Selected awards and special recognition
He was also the first surgeon to perform endovascular harvesting of the saphenous vein in Colombia in 1997. He received second place for a poster presentation based on this technique at the Colombian Congress of Cardiology and Cardiovascular Surgery, Cartagena, 8 to 11 February 2006.
He received the Cesar Uribe Piedrahita Medal from the Colombian Medical Federation and the Antioquia Medical College in 2003 for academic and clinical excellence, in addition to several other awards for academic achievement.
He was the chapter president of the Colombian Society of Cardiovascular Surgery and the Colombian Surgical Consensus for multiple terms. He was also the Chairman, and Medical Advisory of the first Latin American Forums on cardiovascular surgery.
He has received several awards including “The best of 2006” from Hospital General de Medellin for his assistance in the development, creation and commissioning of the cardiovascular services unit at that facility. He has also presented his work at numerous national and international conferences.
He speaks English in addition to his native Spanish.
Dr Sergio Franco
San Vicente Fundacion
Cardiovascular Surgery
Medical Director, Cardiopulmonary and Vascular Surgery
While I requested a visit to the operating room, an invitation was not forthcoming.
Selected writings of Dr. Sergio Franco
Book chapters:
1. Franco S., Restrepo G. Momento Quirúrgico óptimo en el paciente con enfermedad valvular cardiaca. Libro Tópicos selectos en enfermedades cardiovasculares 2000. Unidad cardiovascular Clínica Medellín. 1 Edición. Página. 101-112. ISBN 958-33-1541-9
2. Franco S. Endocarditis Infecciosa: Visión Quirúrgica – Indicaciones de Cirugía. Libro Tópicos selectos en enfermedades cardiovasculares 2000. Unidad cardiovascular Clínica Medellín. 1 Edición. Páginas 201-211. ISBN 958-33-1541-9
3. Franco, S. Estenosis Mitral – Tratamiento Quirúrgico. En: Franco, S. (Ed) Enfermedad valvular cardiaca. Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 111-116 Abril 2001. ISBN : 958-33-2244-X
4. Franco, S., Giraldo, N. , Vélez JF. Uso e Indicaciones deHomoinjertos – Cirugía de Ross. En: Franco, S (Ed) Enfermedad Valvular Cardiaca. Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 70 – 77, Abril 2001. ISBN : 958-33-2244-X
5. Alzate L., Franco S. Factores hemodinámicos y físicos de las válvulas cardiacas artificiales. En: Franco, S. (Ed) Enfermedad Valvular Cardiaca – Sociedad Colombiana de Cardiología. Editorial Colina, 1 edición, Pgnas 222 – 228 Abril 2001. ISBN : 958-33-2244-X
6. Franco, S., Vélez, J. Revascularización Quirúrgica del Miocardio: Estado actual. En: Tópicos selectos en terapéutica cardiaca y vascular 2001. Cardiología Clínica Medellín. P: 108 –120. Primera edición, Octubre 2001. ISBN : 958-33-2607-0
7. Vélez, JF, Franco, S., Tamayo L. Tratamiento quirúrgico de la enfermedad coronaria. En: Enfermedad Coronaria. Pineda M, Matiz H, Rozo R. (Ed), septiembre 2002. Capitulo 36, pgnas 609-630. ISBN : 958-33-3945-8
8. Franco, S.Intervencion Quirúrgica de los síndromes coronarios agudos. En: Tópicos selectos en enfermedades cardiovasculares, 2002. Pgna 177-192 (Velásquez D, Uribe W, editores) Ed. Colina, Departamento de Cardiología Clínica Medellín 2002. ISBN 958-33-3663-7
9. Franco, S.Cardiopatías Congénitas del Adulto. En: Tópicos selectos en cardiología de consultorio 2003. Pgnas 193-211. (Restrepo G., Uribe W., Velásquez D., editores). Ed. Colina, Cardiología Clínica Medellín, 2003. ISBN : 958-33-4858-9
10. Franco, S.Enfermedad Valvular Cardiaca: Indicaciones de Cirugía. En: Libro II Congreso medicina cardiovascular y torácica. . Hospital Departamental Santa Sofía de Caldas, 2003 (Jaramillo O., Editor) Editorial Tizan. Pgnas 87-104
11. Franco, S.Tratamiento Quirúrgico de la Fibrilación Atrial. En: Libro II Congreso medicina cardiovascular y torácica. Hospital Departamental Santa Sofía de Caldas, 2003. (Jaramillo O., Editor) Editorial Tizan. Pgnas 123-131
14. Franco, S., Giraldo, N. Tratamiento Quirúrgico del Paciente Valvular en Falla Cardiaca. En: Enfermedad Valvular Cardiaca. Paginas 169 – 176. (Franco, S., Editor). Editorial Colina. Primera Edición 2004. 227 paginas. ISBN 958-33-6218-2
15. Franco, S. Jiménez A. Factores Físicos y Hemodinámicos de las Prótesis Valvulares Cardiacas. En: Enfermedad Valvular Cardiaca. Pgnas 223-227. (Franco, S., Editor). Editorial Colina. Primera Edición 2004. 227 paginas. ISBN 958-33-6218-2
16. Franco, S.Guías de manejo de las valvulopatias aorticas. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2004. Pgnas 143-149. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2004. 195 paginas. ISBN 958-33-6285-9
17. Franco, S.Guías de manejo de las valvulopatias mitrales. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2004. Pgnas 149-155. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2004. 195 paginas. ISBN 958-33-6285-9
18. Franco, S.Tratamiento Quirúrgico de la Fibrilación Atrial. En: Falla Cardiaca, Diagnostico y manejo Actual. 2004. Pgnas 271- 287.. (Castro, H; Cubides, C. Editores) Editorial Blanecolor, Primera edición, 2004. 431 pgnas. ISBN 33-6689-7
19. Escobar, A. Franco, S. Trauma de grandes vasos torácicos. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 160- 169. 193 paginas. ISBN : 958-33-7698-1
20. Franco, S., Vélez, A. Trauma cardiaco. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 154- 159. ISBN : 958-33-7698-1
21. Franco, S., Jaramillo, J. Tumores cardiacos. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 117 – 123. 193 paginas. ISBN : 958-33-7698-1
22. Franco, S., Vélez, A. Trauma cardiaco. En: Tópicos Selectos en guías de manejo en enfermedades cardiacas y vasculares – 2005. Manual Condensado. (Velásquez D., Uribe W. editores) 1 Edición, editorial colina, 2005. pgnas 362- 366. 388 paginas. ISBN : 958-33-7698-1
23. Franco, S.Guías de manejo de las valvulopatias aorticas. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2005. Manual condensado. Pgnas 177-182. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2005. 388 paginas. ISBN : 958-33-7698-1
24. Franco, S.Guías de manejo de las valvulopatias mitrales. En: Tópicos Selectos en Guías de Manejo en Enfermedades Cardiacas y Vasculares 2005. Manual condensado. Pgnas 183-188. (Uribe, W, Velásquez D, Restrepo G., Editores). Editorial Colina. Primera edición, 2005. 388 paginas. ISBN : 958-33-7698-1
25. Jaramillo, J.S., Franco, S.Implante Quirúrgico del Electrodo Epicárdico en el Ventrículo Izquierdo Mediante Cirugía. En: Duque, M., Franco, S. Editores. Tratamiento no Farmacológico de la Falla Cardiaca. Sociedad Colombiana de Cardiología y Cirugía Cardiovascular. Primera Edición, Editorial Colina, Pgnas 89-92, Abril 2006. ISBN : 958-33-8661-8
26. Franco, S.Cirugía de Remodelación Ventricular en Falla Cardiaca. En: Duque, M., Franco, S. Editores. Tratamiento no Farmacológico de la Falla Cardiaca. Sociedad Colombiana de Cardiología y Cirugía Cardiovascular. Primera Edición, Editorial Colina, Pgnas 168 – 182, Abril 2006. ISBN : 958-33-8661-8
27. Jaramillo, JS., Franco, S., Vélez, JF. Revascularización Coronaria Quirúrgica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 559-576. ISBN : 958-33-9493-9
28. Franco, S., Vélez, JF, Jaramillo, JS., Cirugía en Enfermedad Valvular Aortica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 588 – 595. ISBN : 958-33-9493-9
29. Franco, S., Vélez, JF, Jaramillo, JS., Valvulopatia Mitral. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 596 – 603. ISBN : 958-33-9493-9
30. Franco, S., Vélez, JF, Jaramillo, JS., Cirugía en Enfermedad Valvular Pulmonar y Tricúspidea. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 604 – 606. ISBN : 958-33-9493-9
31. Jaramillo, JS., Franco, S., Vélez, JF, Disección Aortica. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 607 – 617. ISBN : 958-33-9493-9
32. Franco, S., Vélez, A., Trauma de Corazón y Grandes Vasos. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 618 – 625. ISBN : 958-33-9493-9
33. Franco, S., Jaramillo, JS., Vélez, JF., Tumores Cardiacos. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 626 – 635. ISBN : 958-33-9493-9
34. Vélez, JF, Franco, S., Jaramillo, JS., Cardiopatías Congénitas del Adulto. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 649 – 659. ISBN : 958-33-9493-9
35. Uribe, W., Franco, S., Gil, E. Fibrilacion Auricular. En: Velásquez, D., Restrepo, G., Duque, M., Uribe, W., Franco, S. Editores. Tópicos Selectos En Enfermedades Cardiacas y Vasculares – 2006, Estado del Arte. Primera Ed, 2006, Editorial Colina. Pgnas 441 – 466. ISBN : 958-33-9493-9
36. Restrepo, G., Franco, S.Endocarditis Infecciosa. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo VI, pgnas 614-30. ISBN : 958-97065-7-6
37. Franco, S., Sandoval, N. Tratamiento Quirurgico de la Fibrilacion Atrial. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo IX, pgnas 835-842. ISBN : 958-97065-7-6
38. Franco, S., Jaramillo JS. Trauma Cardiaco. En : Texto de Cardiologia. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. Legis, S.A. 1 Ed, 2007; Capitulo XVI, pgnas 1442-49. ISBN : 958-97065-7-6
39. Franco, S., Velez, A. Trauma Vascular Cervical. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 31, P 425 – 433. ISBN : 979-958-98111-9-1
40. Franco, S., Velez, A., Jaramillo JS. Trauma Cardiaco. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 30, P 419 – 423. ISBN : 979-958-98111-9-1
41. Franco, S.Guias de Manejo de las Valvulopatias Aorticas. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 25, P 379 – 385. ISBN 978-958-98111-9-1
42. Franco, S.Guias de Manejo de las Valvulopatias Mitrales. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin; 2007. Capitulo 26, P 387 – 392. ISBN : 979-958-98111-9-1
43. Jaramillo, J.S., Franco, S.Guias de Manejo de la Revascularizacion Coronaria Quirurgica. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares 2007. Manual Condensado, 3 Edicion, Cardiologia Clinica Medellin. Capitulo 24, P 369 – 377. ISBN : 979-958-98111-9-1
44. Franco, S.; Velez, JF.; Jaramillo,JS. Complicaciones mecanicas del infarto agudo del miocardio. En : Topicos Selectos en Enfermedad Coronaria – 2008. Velasquez, D. ed; Distribuna Ed, Cardiologia Clinica Medellin, 2008. P. 115-126. ISBN 978-958-8379-09-8
45. Jaramillo,JS.; Franco, S.; Velez, JF. Guias de manejo de la revascularizacion coronaria quirurgica. En : Topicos Selectos en Enfermedad Coronaria – 2008. Velasquez, D. ed; Distribuna Ed, Cardiologia Clinica Medellin, 2008. P. 197- 218. ISBN 978-958-8379-09-8
46. Franco, S.; Jaramillo, J.S. Guías de Manejo de la revascularización Coronaria Quirúrgica. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 429-440. ISBN : 978-958-8379-19-7
47. Franco, S.; Jaramillo, J.S. Guias de Manejo de las valvulopatias aorticas. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 441-448. ISBN : 978-958-8379-19-7
48. Franco, S.; Jaramillo, J.S. Guias de Manejo de las valvulopatias mitrales. En: Guias de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edicion 2009, 503 paginas. P. 449-456. ISBN : 978-958-8379-19-7
49. Franco, S.; Jaramillo, J.S. Trauma Cardiaco. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edición 2009, 503 paginas. P. 487-492. ISBN : 978-958-8379-19-7
50. Franco, S.; Jaramillo, J.S. Trauma Vascular Cervical. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2009. Velásquez, D. Ed. Editorial Distribuna, 1 edición 2009, 503 paginas. P. 493 – 503. ISBN : 978-958-8379-19-7
51. Franco, S.; Jaramillo, J.S. Trauma Vascular Cervical. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 501 – 511. ISBN : 978-958-8379-29-6
52. Franco, S.; Jaramillo, J.S. Trauma Cardiaco. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edicion 2010, 511 paginas. P. 495 – 500. ISBN : 978-958-8379-29-6
53. Franco, S.; Jaramillo, J.S. Guías de Manejo de las Valvulopatias Mitrales. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 457 – 463. ISBN : 978-958-8379-29-6
54. Franco, S.; Jaramillo, J.S. Guías de Manejo de las Valvulopatias Aorticas. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 449 – 456. ISBN : 978-958-8379-29-6
55. Franco, S.; Jaramillo, J.S. Guías de Manejo de la Revascularización Coronaria Quirúrgica. En: Guías de manejo en enfermedades cardiacas y vasculares. Manual Condensado 2010. Velásquez, D. Ed. Editorial Distribuna, 2 edición 2010, 511 paginas. P. 437 – 447. ISBN : 978-958-8379-29-6
56. Franco, S.; Bucheli, V. Anatomía Quirúrgica de la Válvula Mitral. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 26 – 31. ISBN : 978-958-44-7706-4
57. Franco, S.; Bucheli, V. Anatomía Quirúrgica de la Válvula Aortica. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 33 – 38. ISBN : 978-958-44-7706-4
58. Franco, S. Endocarditis Infecciosa. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 85 – 113. ISBN : 978-958-44-7706-4
59. Franco, S. Criterios para la Selección de una Prótesis Cardiaca. En : Enfermedad Valvular Cardiaca. Franco, S. Ed., Editorial Colina, Primera Edición 2010, 440 paginas. P. 433 – 440. ISBN : 978-958-44-7706-4
60. Franco, S., Atehortua, M. Endocarditis Infecciosa. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 153 – 184. ISBN : 978-958-8379-46-3
61. Franco, S., Atehortua, M. Valvulopatia Mitral. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 717 – 727. ISBN : 978-958-8379-46-3
62. Franco, S., Atehortua, M. Cirugía Valvular Aortica. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 707 – 717. ISBN : 978-958-8379-46-3
63. Atehortua, M., Franco, S. Revascularización Coronaria Quirúrgica. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 675 – 690. ISBN : 978-958-8379-46-3
64. Atehortua, M., Franco, S. Evaluación y Momento Optimo de Intervención en el Paciente con Enfermedad Valvular Cardiaca. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 691 – 707. ISBN : 978-958-8379-46-3
65. Atehortua, M., Franco, S. Cirugía en Enfermedad Valvular y Tricuspidea. En : Estado Actual en Enfermedades Cardiacas y Vasculares 2011. Ed. Editorial Distribuna, 1 Edición 2011, 744 pnas. Pgna 727 – 744. ISBN : 978-958-8379-46-3
66. Atehortua, M., Franco, S., Velez, L.A. Guias de Manejo de Revascularizacion Coronaria. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 619 – 630. ISBN : 978-958-8379-60-9
67. Velez, L.A., Franco, S., Atehortua, M. Guias de Manejo de las Valvulopatias Aorticas. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 631 – 642. ISBN : 978-958-8379-60-9
68. Atehortua, M., Franco, S., Velez, L.A. Guias de Manejo de las Valvulopatias Mitrales. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 643 – 653. ISBN : 978-958-8379-60-9
69. Velez, L.A., Atehortua, M., Franco, S. Cirugia en Enfermedad Valvular Pulmonar y Tricuspidea. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 655 – 661. ISBN : 978-958-8379-60-9
70. Franco, S., Bucheli, V., Atehortua, M., Velez, L.A. Guias de Manejo en Endocarditis Infecciosa En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 671 – 690. ISBN : 978-958-8379-60-9
71. Franco, S., Bucheli, V., Atehortua, M., Velez, L.A. Guias de Manejo de los Sindromes Aorticos Agudos. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 691 – 702. ISBN : 978-958-8379-60-9
72. Franco, S., Atehortua, M., Velez, L.A. Trauma Cardiaco. En : Guias de Manejo en Enfermedades Cardiacas y Vasculares Estado Actual – 2012. Ed. Editorial Distribuna, 3 Edición 2012, 708 pnas. Pgna 703 – 708. ISBN : 978-958-8379-60-9
Journal articles
1. Franco Sergio, Hincapié Miriam, Mejía Olga. Estudio Epidemiológico de Teníasis. Cisticercosis, San Vicente Antioquia – Colombia, 1985-1986. En: Medicina Tropical y Parasitología Vol. 2 No 1, Ecuador, Diciembre 1985.
2. Franco Sergio, Hincapié Miriam, Mejía Olga. Estudio Epidemiológico de Epilepsia y Neurocisticercosis. En: “Revista Universidad Industrial de Santander – Medicina¨ Vol. 14 No 1, Mayo 1986, p 143- 74.
3. Botero D., Franco S., Hincapié M., Mejía O. Investigaciones Colombianas Sobre Cisticercosis. En: Acta Neurológica. Vol. 2 No 2 Septiembre 1986, p. 3-6.
4. Franco Sergio; Londoño Juan. Dermatopoliomiositis – Reporte de un caso – Revisión del Tema. En: Medicina – U.P.B. Vol. 7 No 2, Noviembre 1988. p. 115.
5. Franco Sergio; Vásquez Jesús; Ortiz Jorge. Infarto Segmentario Idiopático del Epiplón Mayor – Presentación de dos casos y revisión del tema. En: Medicina – U.P.B. Vol. 10 No 2. Octubre. 1991, p. 109.
6. Franco Sergio. Choque Hipovolémico. Medicina U.P.B., Vol. 13 No 2, Octubre, 1994. P. 139-160.
7. Montoya A., Franco S.,. Lung Transplantation for Bronchoalveolar Cell Carcinoma. First Case Report in the Word Literature. 1996 – Loyola University Chicago Annual Report Magazine.
8. Franco S. Autopsy Results in Patients Following Lung Transplantation. Department of Pathology at Loyola University Medical Center. 1996 – Loyola University Chicago Annual Report Magazine.
9. Franco S., Giraldo N., Flórez M. Tratamiento Quirúrgico de la Coartación Aórtica Seguimiento a Largo Plazo – 8 años. Revista Colombiana de Cardiología. Vol. 5 No 5, Diciembre 1996.
10. Franco S, Giraldo N. Trauma Cardíaco: Revisión del Tema. Revista Colombiana de Cardiología. Marzo de 1997.
11. Franco S., Giraldo N., Ramírez C., Vallejo C., Castro H. Revascularización Miocárdica en pacientes con fracción de eyección menor del 30%. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 301.
12. Franco S., Giraldo N., Fernández H., Ramírez C., Vallejo C., Castro H. Transección Aórtica Traumática: Presentación de tres casos, revisión de la literatura. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 330.
13. Franco S., Giraldo N., Vélez S. et al. Fístula de la arteria coronaria derecha al tracto de salida del ventrículo derecho. Reporte de un caso – revisión del tema. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 319.
14. Giraldo N., Franco S., Ramírez C., Vallejo C., Castro H. CIV y Banding de la arteria pulmonar en un paciente adulto. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 333.
15. Giraldo N., Franco S., Ramírez C., Vallejo C., Castro H. Ruptura Ventricular post implantación de válvula mitral. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 340.
16. Castro H., Ramírez C., Franco S., Mesa J. et al. Anestesia y técnica quirúrgica en pacientes sometidos a implantación percutánea de endoprótesis en aneurismas de la aorta abdominal. Reporte de tres casos y revisión de la literatura. Departamento de Cirugía y Anestesia Cardiovascular. Departamento de Hemodinámica. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 331.
17. Vallejo C., Castro H., Ramírez C., Franco S., Duque M. et al. Anestesia y técnica quirúrgica en pacientes sometidos a implante de cardiodesfibrilador automático. Reporte de 20 casos. Departamento de Cirugía y Anestesia Cardiovascular. Departamento de Electrofisiología y Arritmias. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
18. Ramírez C., Vallejo C., Castro H., Franco S., Giraldo N. et al. Protección Miocárdica: Solución de HTK en Cirugía Cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
19. Ramírez C., Vallejo C., Castro H., Franco S., Giraldo N. et al. Protección Miocárdica: Comparación entre la Solución de HTK y la Solución de Buckberg en Cirugía Cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 336.
20. Vallejo C., Ramírez C., Castro H., Giraldo N., Franco S. Hipotiroidismo y enfermedad cardiaca: Administración de hormona tiroidea vía oral en pacientes sometidos a cirugía cardiaca. Departamento de Cirugía y Anestesia Cardiovascular. Unidad Cardiovascular Clínica Medellín. XVIII Congreso Colombiano de Cardiología. Medellín, 1999. Revista Colombiana de Cardiología, 1999, Vol. 7(6): 334.
21. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Revascularización miocárdica con arteria radial: Estudio de Casos y Controles. Departamento de Cirugía Cardiotorácica, Clínica Medellín. XIX Congreso Colombiano de Cardiología. Noviembre 27 – Diciembre 1, 2001. Revista Colombiana de Cardiología, 2001, Vol. 9(2): 197.
22. Giraldo, N., Franco, S., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Revascularización miocárdica Off Pump: Requerimiento de derivados sanguíneos. Departamento de Cirugía Cardiotorácica, Clínica Medellín. XIX Congreso Colombiano de Cardiología. Noviembre 27 – Diciembre 1, 2001. Revista Colombiana de Cardiología, 2001, Vol. 9(2): 238.
23. Giraldo, N., Franco, S. Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Endarterectomia Coronaria del tronco principal izquierdo. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES Medicina Vol. 16 # 1, página 39-44. Enero-Marzo 2002.
24. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Cierre tardío del esternón en el manejo del sangrado mediastinal post cirugía cardiaca. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES – Medicina. Vol. 16 # 1, página 27-34. Enero-Marzo 2002.
25. Franco, S., Giraldo, N., Fernández H., Escobar A., Ramírez, C., Vallejo, C., Castro H. Cambio valvular mitral con preservación total del aparato valvular: Técnica quirúrgica, resultados y seguimiento. Departamento de Cirugía Cardiotorácica, Clínica Medellín. CES Medicina. Volumen 16 # 1, página 9-18. Enero-Marzo 2002.
26. Franco S, Giraldo N, Escobar A, Fernández H, Vallejo C, Ramírez C. Cambio valvular mitral con preservación total del aparato valvular: técnica quirúrgica, resultados y seguimiento. Revista Colombiana De Cardiología. 2003. pp. 368 – 74
27. Giraldo N, Franco S, Escobar A, Fernández H, Vallejo C, Ramírez C. Cierre tardío del esternón en el manejo del sangrado mediastinal post cirugía cardiaca. Revista Colombiana De Cardiología 2003. pp. 95 – 99
28. Escobar A., Giraldo N., Franco S., Jaramillo J., Orozco A. Taquiarritmias supraventriculares postcirugia cardiaca con y sin el uso de circulación extracorpórea. En : CES Medicina Volumen 17 # 1, Enero-julio 2003, Pgnas 23-31
29. Echeverri JL, Gonzáles M, Franco S., Vélez LA. Ruptura traumática de la aorta. Reporte de dos casos y revisión de la literatura. Medicina Crítica y Cuidados Intensivos. Enero – Junio 2004, 2 (1) : 31-35
30. Franco, S. Giraldo, N., Gaviria, A. et al. Aneurismas y seudoaneurismas de injertos venosos coronarios. Revista Colombiana de cardiología, Vol. 11 # 8, Abril 2005. Pgna 401- 404.
31. Franco, S.; Uribe, W.; Velez, JF. et al. Tratamiento quirurgico curativo de la fibrilacion atrial mediante tecnica de ablacion con radiofrecuencia monopolar irrigada : resultados a corto y mediano plazo. Revista Colombiana de Cardiologia. 2007. Vol 14, # 1. Pnas 43 – 55.
32. Escobar, A., Franco,S., Giraldo,N., et al. Tecnica de perfusion selectiva cerebral via subclavia para la correccion de patologias del arco aortico. Revista Colombiana de Cardiologia Volumen 14, numero 4, agosto 2007. P 232-237
33. Franco, S.Tratamiento quirurgico de la fibrilacion atrial. Revista Colombiana de Cardiologia – Guias de Diagnostico y Tratamiento de la Fibrilacion Auricular. Vol 14, Suplemento 3, Octubre 2007. P. 133 – 143.
34. Franco, S. Velez, A., Uribe, W., Duque, M., Velez, JF, et al. Tratamiento quirurgico de la fibrilacion atrial mediante radiofrecuencia. Revista Medica Sanitas 2008, Volumen 11, Numero 1, pgnas 8 – 20. Febrero – Abril, 2008.
35. Franco,S., Herrera, AM., Atehortua, M. et al. Use of Steel bands in sternotomy closure : implications in high-risk cardiac surgical population. Interactive CardioVascular and Thoracic Surgery 8 (2009) : 200-205.
36. Franco, S.Tratamiento Quirurgico para el manejo de las arritmias ventriculares. Guias Colombianas de Cardiologia. Artitmias Ventriculares y Muerte Subita. Revista Colombiana de Cardiologia. Volumen 18, Suplemento 1. Pgnas 160 – 163. Febrero 2011.
37. Miranda, A. ; Franco, S.,; Uribe, W. et al. Tromboembolismo Pulmonar Masivo de Alto Riesgo. Medicina ( Buenos Aires), 72 : 2012; Pgnas 128-130.
38. Miranda, A., Duque, M., Franco, S., Velasquez, J. et al. Tromboembolismo Pulmonar Masivo. Indicaciones de Cirugia – Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1. Marzo de 2012.
39. Franco, S.; Eusse, A.; Atehortua, M., Vélez, L., et al. Endocarditis Infecciosa : Análisis de Resultados del Manejo Quirúrgico Temprano. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 66. Marzo de 2012.
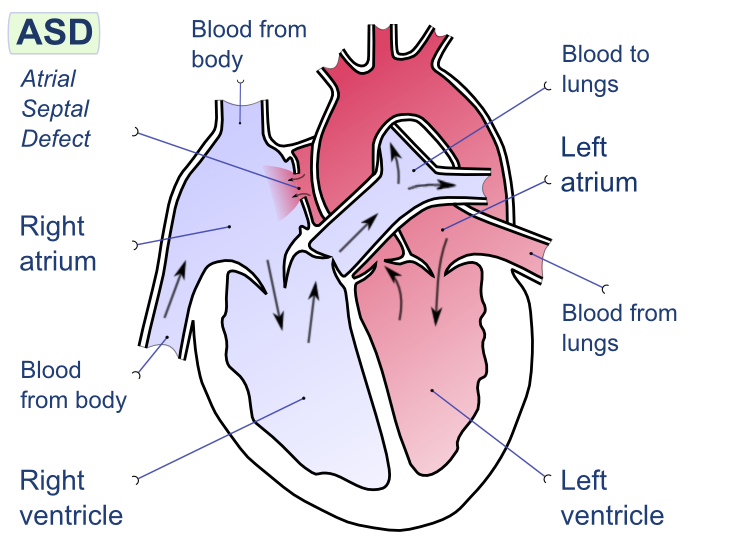
40. Franco, S.; Bucheli, V.; Atehortua, M., Vélez, L.; Eusse, A et al. Tratamiento Quirurgico : El “Gold Estándar” en el manejo de los defectos del septum interauricular. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1. Marzo de 2012.
41. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., et al. Anomalías coronarias del Adulto. Origen anómalo de la arteria coronaria izquierda de la arteria pulmonar (ALCAPA). Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 61. Marzo de 2012.
42. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., et al. Metástasis cardiaca de carcinoma anaplasico de tiroides. Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 70. Marzo de 2012.
43. Franco, S.; Giraldo, N.; Atehortua, M., Vélez, L.; Castro, H., et al. Endarterectomia coronaria del tronco principal izquierdo : Seguimiento a 15 años. Reporte de caso. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 66. Marzo de 2012.
44. Franco, S.; Atehortua, M., Vélez, L.; Castro, H., Bucheli, V.; et al. Implante de válvulas biológicas : evaluación de libertad de reoperación por deterioro valvular estructural. Revista Colombiana de Cardiologia. Volumen 19, Suplemento 1, pgna 69. Marzo de 2012.
45. Miranda, A. Franco, S. Uribe, W., Duque, M. et al. Tromboembolismo Pulmonar Masivo de Alto Riesgo Asociado a Foramen Ovale Permeable. Medicina (Buenos Aires) 72 : 128 – 130. 2012.
46. Franco, S.Criterios Para la Selección de Una Protesis Cardiaca. Rev Fed Arg Cardiol. 2012; 41(3): 156 – 160.
Special topics in Cardiac Surgery: (Monographs)
1. Franco Sergio. Manejo Básico Inicial del Paciente Con Trauma CortoPunzante En: Monografía. Hospital San Vicente de Paúl – Prado (Tolima) 1989.
2. Franco S; Montoya A. Transplante Pulmonar: Indicaciones, Criterios de Selección y rechazo, Técnica Quirúrgica, Manejo de Donante y receptor, Complicaciones. Protocolo para la realización de transplante pulmonar en nuestro medio. Comité de transplantes de corazón y pulmón. 1996. Clínica Cardiovascular Santa María, Biblioteca Médica – Facultad de Medicina, Universidad Pontificia Bolivariana
3. Giraldo N., Franco S., Estudiantes X Semestre Instituto de Ciencias de la Salud – CES. Tratamiento Quirúrgico de la Endocarditis Infecciosa. Monografía. Investigación realizada en la Clínica Cardiovascular Santa Maria. Publicación Monográfica. Enero 1997.
4. Franco S. Safenectomía Videoendoscópica. Realización de video con descripción de la técnica quirúrgica. Descripción Monográfica. Departamento de Cirugía Cardiovascular. Unidad Cardiovascular Clínica Medellín. Diciembre de 1997.
5. Franco S., Giraldo N., Fernández H. Tratamiento Quirúrgico de la Enfermedad Pulmonar Obstructiva Crónica. Cirugía de Reducción de Volumen Pulmonar. Monografía, Departamento de Cirugía Cardiovascular – Unidad Cardiovascular Clínica Medellín. Octubre 1999.
6. Franco S., Escobar A. Trauma de Tórax. Revisión del tema. Monografía. Departamento de Cirugía Cardiovascular / Unidad Cardiovascular Clínica Medellín. Octubre de 1999.
7. Franco S., Jaramillo J.C. Cirugía en el paciente con Angina. Consenso Nacional sobre el Manejo de la Angina de Pecho. Sociedad Colombiana de Cardiología. Bogota, 11-12 agosto 2000.
8. Franco, S. Fibrilación Atrial: Tratamiento Quirúrgico. I Actualización del Consenso Nacional Sobre Fibrilación Atrial. Capitulo de Electrofisiología, Sociedad Colombiana De Cardiología. Abril 2002.
9. Franco, S, Jaramillo JS, Vélez JF, Castro H. Infecciones Mediastinales. Monografía. Departamento de Cirugía Cardiovascular. Hospital Departamental Santa Sofía de Caldas, Manizales. Mayo de 2003.
10. Guias Colombianas de Cardiologia. Fibrilacion Atrial – Guias de bolsillo.
Duque, M, Marin, J, ed. Franco, S. Cirugia de fibrilacion atrial. Sociedad Colombiana de Cardiologia y Cirugia Cardiovascular. 2008.
11. Franco, S. Long-Term Effectiveness of HIFU on Atrial Fibrillation in High Risk Valvular Surgery Patients. A Clinical Interview from Epicor- Cardiac Ablation System – St Jude Medical. March 2009.
What is the difference between a medico estetico and a cirujano plastico? The answer is more than just an issue of translation and semantics. We discussed this and several other issues during a visit to Clinica Plastic & Estetica Nova with Julio Casadiego, who works in the medical tourism sector here in Medellin at Colombia Travel Operator. Mr. Casadiego works with many of the healthcare professionals here in Colombia to assist overseas traveler in making arrangements for medical travel and has done so since 2009.
The Clinica Plastica & Estetica NOVA
Carrera 48 #32B sur 30
Envigado, Antioquia
Tele: (4) 339 2300 EXT 125
Email: gerencia@clinicanova.com.co
Nova is an ambulatory surgery center and a center for aesthetics. (Aesthetics is an umbrella term that encompasses other treatments outside of plastic surgery.) This five-story facility houses several doctors offices, aesthetic treatment facilities (laser treatment area) other nonsurgical treatment areas (cellulite treatment, botox/ injectables etc.), a cosmetic dentist (Dr. Jorge Ivan Echavarria) specializing in crowns, dental implants, maxiofacial surgery, and orthodontics along with other cosmetic services such as teeth-whitening.
There is a small pharmacy as well as a full lab (for development of gel matrix in addition to performing blood analysis), and sterilization facilities along with an operating theatre and recovery unit.
There are three operating rooms; all of which are spacious and well-lit. Each operating room has a full complement of fully functional and modern equipment and hemodynamic monitoring devices. There are also several well placed ‘crash carts’ for potential emergencies. The recovery room contains hemodynamic monitoring equipment with additional emergency equipment (just in case.) Dr. Diego Correa was my guide for a tour of the operating facilities and was happy to answer all of my questions.
He also reported that in the last year there have been just three cases of minor skin infections (the causative agent was normal skin flora). He reports no serious infections or complications after surgery, and states that have been no instances of resistant bacteria or MRSA.
What is a Medico Estetico?
The literal translation of medico esthetico is aesthetics doctor, but a more accurate description would be a doctor who serves as an Aesthetics Consultant, or a doctor who performs nonsurgical aesthetics treatments. For a better understanding of this specialty, I spoke with Dr. John Jairo Monsalve Bedoya, a medico estetico and general director at the Nova clinca.
A cirujano plastico is a ‘plastic surgeon’. This is the surgeon who is trained to perform surgical procedures such as abdominoplasties, breast augmentation and similar types of procedures.
As he explained, the Aesthetics Doctor is a physician who specializes in the study of Aesthetic procedures. Patients consult with this physicians as part of the initial consultation to help patients determine what procedures the patient needs or wants to achieve a desired result. This is important in many cases when the patient knows what type of result they want (“I want to look younger”, for example) but may not know exactly what procedure is best to accomplish the results they want.
During the consultation, the doctor listens to the patient describe what they are looking for, collections medical history and other medical information as well as preferences. Then the doctor discusses a range of procedures from injectables (botox, restalyne, gel matrix), and other non-surgical treatments (laser/ light therapies, mini-lift procedures) to larger, more invasive surgical procedures such as facial endoscopy, traditional face-lifts, eye lifts and other related procedures.
Finally, based on the information provided and the discussion with the patient and their family – the doctor recommends the procedures to accomplish the results the patients are seeking.
Once the patient has decided on their options, Dr. Monsalve, and his associate Dr. Correa begin the pre and post-operative treatment plan. This plan is more than discussing payment, arranging a date for surgery, and a follow-up visit. As Dr. Monsalve explains – it’s a process that encompasses the entire pre-operative period, surgery and recovery.
Patients undergo a compete physical examination, with blood work and cardiac testing as appropriate (usually EKG). Patients are evaluated and treated by internal medicine physicians for any co-morbid conditions before meeting with the anesthesiologist for further evaluation. (This is done to reduce risk of peri-operative and post-operative complications). The degree of pre-surgical evaluation is related to the type of treatment – with more comprehensive evaluations for patients who elect to have surgical procedures with general anesthesia.
Intra-operative care is provided by the attending anesthesiologist with the initial post-operative recovery under monitored care in the recovery room. But after the immediate recovery, patients aren’t simply discharged home.
The discharge planning / recovery phase is also governed by Dr. Monsalve and his team. This includes a 24 hour call line, and home visits, as needed. In fact, Dr. Monsalve encourages patients to call, saying, If a patient is having pain – they should call.. If they have questions or concerns, they should call. It doesn’t matter what time it is.
Dr. Monsalve also encourages patients to consider aesthetics “a process- not just a surgery”. He states that this treatment is a part of a patient’s life, and that using a philosophy of a process-based approach (rather than an episodic experience of pay – surgery – follow-up visit) results in a better patient experience, better outcomes and greater satisfaction/ happiness with the outcomes. He believes that successful aesthetic procedures aren’t about making people prettier, it’s about making people happier with themselves.
Medellin surgeons serving their community
During our discussion, we also talked about the many ways that local surgeons give back to their communities. While this includes the more widely known programs such as Operacion Sonrisa, it also includes programs such as Gorditis de Corazon for post-bariatric procedures, Angeles por Colombia , a more generalized organization that recruits volunteers from all professions and areas of society (which operates under a philosophy of each one recipient then helps three others) as well as several other programs aimed at providing reconstructive surgery procedures to low-income Colombians.
Gel Matrix for skin rejuvenation
During our visit we also talked to Dr. Maria del Pilar Sanin, another medica estetica, who performs many of the non-surgical procedures offered at Nova. She talked about Recombinant Plasma (approximate translation) which uses a gel matrix made for the patient’s own blood to improve the appearance and condition of the skin.
The origins of gel matrix: cardiac surgery
Having worked in cardiac surgery, this concept is not new – our perfusionist in Virginia often used the patient’s shed blood in orthopedic surgery to make a similar gel matrix that enhanced healing and reduced inflammation – particularly in patients with a history of poor wound healing.
Here at the clinica Nova, no major surgery is required. Blood is taken, (by syringe) and placed into a centrifuge. Now if you can remember back to high school biology – this causes the blood to separate into its components, buffy coat, platelets and red cell matter. Then the doctor uses the platelet rich portion (which also contains fibroblasts, collagen, and other nutrients important to skin elasticity and wound healing). This formula is then injected in small increments into the patient’s face to promote skin health and rejuvenation. Since the material is made for the patient’s own body, (and unadulterated with preservatives or other chemicals) there is no possibility for allergic reactions or sensitivities to the ingredients.
Dr. Maria del Pilar Sanin reports that the healing time for this procedure is approximately four days, and that redness and inflammation at the sites of injections are common immediately after this procedure. She states that the duration of the effects depend on the patient’s underlying skin condition, general health and age. On average it lasts 1.5 to 2.0 years in most patients, but may not last as long in patients with extensive sun damage or deteriorated skin condition.
She recommends this procedure as a complimentary treatment to other non-surgical treatments for better overall skin condition/ health and a reduction in the appearance of wrinkles and fine lines. She reports it is frequently used to treat the deepening of the naso-labial fold (the line that stretches from the nose to the corners of the mouth.)
Clinica Nova offers a wide-range of patient-centered aesthetic procedures and plastic surgery – all under one roof.
Medellensa (or women from Medellin) are considered some of the most beautiful women in the world. However, they often have had some help. Plastic surgery is wildly popular in Medellin, Colombia and much of Latin America, and standards of beauty are based on a voluptuous physique with large breasts, small waist and an (often) exaggerated caboose. Actress Sofia Vergara, of Barranquilla is a classic example of Colombian beauty ideals, which have spread into popularity to the United States. Many North Americans and Europeans seeking this look come to Medellin for the city’s famed plastic surgeons.
Of the 650 members of the Colombian Society of Plastic, Aesthetic and Reconstructive Surgery, 98 members are located in the Medellin area. Using this directory, I attempted to contact surgeons for interviews. When e-mail addresses were not available, I contacted surgeons thru the Colombian Society website, when that option was available*. If the surgeons listed a website, contact was also attempted via website.
Alphabetical listing – compilation is ongoing as I continue efforts to contact and interview plastic surgeons in the city.
Lists English and French in addition to Spanish. Following correspondence, I interviewed Dr. Botero at his office. The interview with Dr. Botero can be seen here. You can read about my visit to the operating room here.
No email listed, emailed through society website on 7/8*.
Profile states he speaks English and Portuguese in addition to Spanish.
Lists plastic surgery education at Hospital Barata Riverio – Rio de Janiero, Brazil.
Martha Elena Gomez Botero
Calle 2 Sur # 46 -55
Clinica Las Vegas
Medellin
Tele: 268-3818
Email: megomezbotero@hotmail.com
Emailed 7/8.
Dr. Gomez specializes in maxiofacial surgery and hand surgery.
** the website email form for the Colombian society of plastic surgeons does not appear to be working. I have contacted the society regarding this issue.
Sundays in Colombia are special to me. The tradition family day of relaxation and enjoyment has existed for centuries but somehow managed to pass me by for most of my adult life. In hospitals, patients need care every single day; on Christmas, on Thanksgiving, the fourth of July and on Sundays.. Usually I am first in line to volunteer to work these days.
I know that these days are important for my co-workers with small children and local family, and I don’t mind working during the holidays; the operating rooms are closed – everything slows down, so it’s a chance to spend some extra time with my patients.
But here in Colombia, I am a writer first, nurse second – so my schedule is very different. No more Sunday rounds, and bedside visits..
Sundays have become a ‘family day’ for me at this late date. A day to enjoy my surroundings, time with family and friends and to experience the food of Colombia.
Today we spent most of the day just outside the city in Parque Arvi. Just the trip to the park is fun – on the metrocable (the city’s tram system) up into the hills of Medellin..
on the metrocable, climbing the hills of Medellin
Then another tram ride across the mountains to the park.
some friends we made on the tram up
The view is glimpse down at a tiny slice of Medellin life..
kids enjoying the pool in the barrio beneath the metrocable
In general, the higher into the hills of Medellin, the poorer the settlements (but not always – some of the nicer estates in Poblado hug the hills on the way to Envigado).
houses hugging the hills of Medellin
But the views of the city itself are spectacular.
the city of Medellin as seen from the tram
It wasn’t a long ride – just long enough to meet our fellow tram riders (each tram holds eight people) including a newly wed couple from Bogotá..
The park itself is lovely, and the temperature just a wee cooler. Lots of families were out enjoying the park and the numerous restaurants selling regional Colombian cuisine. The trip is one of the most popular tourist activities for visitors to Medellin – and I am glad I finally took the time to see for myself.
If you want to understand and to really know life in Medellin, than you need to see the richness and complexities of life here. It’s simplistic to say that life here is more than black and white. It isn’t varieties of grey either.. There are so many levels, and sublevels and little pockets / slices of life here. Every barrio has its own personality; community, strengths and weaknesses.
Never has that been more apparent than during my visit to El Tesoro yesterday to interview Dr. Botero. Even so, I would be selling the city short if I pretended that I truly understood Medellin in my brief time here. My friend, Adriaan has lived here since 2008 and he would be the first person to admit – that it takes much of that time just to scratch beneath the surface.
One of the reasons I write about Colombian life so frequently, in addition to medical issues is to better understand life here – and to share that with my readers. It’s not just another language, or another Latin American country. Superficial differences are great for picture postcards and brief visits – but if you spend any real time here, or want to have lasting business relationships or friendships with people here, than you have to dig deeper (not just into Colombia, but in yourself).
One of the lessons has to do to with what we bring to other countries. A lecturer at the Global Health Conference in Duke one year explained it best. He went on a ‘medical mission’ to Mongolia.. And he thought he should teach them American principles of surgery. But when he got there he talked to the surgeons there and realized they didn’t want or need this. They wanted to learn more about laparoscopic surgery. So he changed his project entirely, and taught laparoscopic surgery. (Notably, he was the only speaker at this three-day conference who listened – and taught what the hosts wanted to learn.)
This is not a medical mission, it’s the anti-thesis to what I do. But I still have to listen, and to consider Colombians and Colombia as a big part of what I do. I am not an imperialist, and I am not a big multi-national organization. But if I am going to encourage people to see Colombia as a viable option to affordable surgery, then I need to consider the Colombians that will be impacted by this.
I have to take time to make sure that my efforts don’t undermine the needs of Colombian citizens – that they don’t lose access to health care providers in favor of the ‘wealthy gringos’ with cold hard cash in hand. I have to try to encourage others in this industry to do the same; to work within the existing framework to try to ensure services for all.
This means that I tend to steer clear of facilities created only for ‘rich gringos’ and send people to the excellent public and private facilities that also serve Colombian citizens. This prevents the diversion of resources away from the very people who live here and rely on these services for everyday life. It means sending people to Fundacion Cardioinfantil, Clinica San Rafael or the National Cancer Institute for the wonderful doctors who work there, instead of the ‘Medical Cities” that are popping up almost daily. That way, these excellent providers continue to serve their communities and the money from medical tourism enriches these same communities instead of the pockets of a very few. These facilities then add services – for everyone. There are enough excellent facilities here that it’s an easy choice – but people traveling to other countries like Thailand and India need to think about this. These countries already suffer from a “brain drain” as their most talented health care providers flock to the ultra-expensive and ultra-elite facilities for wealthy travelers (and leave their own citizens out in the cold.)
There is talk of building several of these tourist hospitals in the coastal cities (Cartagena, Barranquilla and Santa Marta) and I hope it doesn’t come to pass. It would change, and damage this country which I have come to love so much.
This is also why I steer clear of transplant tourism – which is inherently unfair.
Being in Colombia has changed me, because it makes me question a lot of the things that I held as ‘facts’ merely due to my upbringing and geographic orientation. But I feel this is essential for becoming a more intelligent and informed person and citizen of the world. Sometimes it is just noticing the obvious – like the view from the mall at El Tesoro.. Sometimes its taking a minute to talk to the vendors in the park; to listen to their dreams, hopes, worries as well as get their perspectives on life, global and local events. But sometimes its just being here.
All plastic surgeons listed (for Colombia) are members of the Colombian Society of Plastic, Aesthetic and Reconstructive Surgery.
Dr. Luis Botero during a tour of the new El Tesero ambulatory surgery clinic
Dr. Luis Fernando Botero Gutierrez
Carrera 25A #1 -31
Edificio Parque emp. El Tesoro
Office # 907
Medellin, Colombia
Tele: 448 – 6030
Email: luchobot@gmail.com
Website:currently under revision
It is fitting that one of Medellin’s most prominent plastic surgeons shares the same last name as one of Colombia’s most (but not related) famous artists – since plastic surgery requires considerable artistic vision from its practitioners. While Fernando Botero’s classic works depict a more fleshy, voluptuous and sumptuous view of the world, Dr. Luis Botero spends much of his time doing the opposite: slimming and smoothing his clients with the judicious application of the latest liposuction techniques.
Quirofanos El Tesoro
His office is located next to the El Tesoro mall, in one of the most affluent parts of the city, but that will soon change with the August opening of a large ambulatory surgery clinic within the upscale shopping center. Dr. Botero is a large part of the vision behind the 15-million dollar surgery center, which will also house the 150 physician offices from multiple specialties (including 21 plastic surgeons).
Trilingual surgeon
Dr. Botero speaks English and French fluently in addition to his native Spanish. Much of this is due to his training. After attending medical school at the Universidad de Antioquia here in Medellin and practicing as a general medicine physician for four years – he headed to Europe for specialty training in plastic surgery.
He attended the Free University of Brussels (Universite Libre de Bruxelles) in Belgium for his plastic surgery residency before moving to the University Henri Poincare (now University of Lorraine) in Nancy, France for four years to complete fellowships in maxiofacial surgery, plastic surgery of the face and separate training in hand and microsurgery and upper limb surgery. He spent an additional year working as a plastic surgeon in France. He also spent time in Singapore (National University Hospital) with Dr. Robert Pho and Taipei, Taiwan (Chang Gung Memorial Hospital) as a visiting fellow.
He returned to Colombia 12 years ago, and has been working as a plastic surgeon in Medellin ever since.
He is currently the president of the Antioquia chapter of the Colombian Society of Plastic, Aesthetic and Reconstructive surgery as well as holding memberships in Belgian Society of Plastic Surgery and the Group for the Advancement of Microsurgery (GAM). He is also a member of the International Society of Aesthetic Plastic Surgery (ISAPS) and the Latin American Federation of Plastic Surgery (FILACP).
He is the official physician for the French Embassy office in Medellin.
Current practice in Medellin
Despite his extensive training, his current practice is almost exclusively aesthetic surgery (rather than reconstructive, micro or hand surgery). He performs a combination of facial and body procedures including facial endoscopy, and reports that like almost all plastic surgeons, around fifty percent of his practice is liposuction.
While the majority of his practice are women, he estimates that around 15% are male clients. The most popular procedure for his male patients are blepharoplasty (eye-lid lift), mandibular liposuction (chin) and corporal liposuction (body).
He is patient, pleasant and very likeable. We talk about current trends in plastic surgery, cultural attitudes regarding plastic surgery and the anticipated opening of the new clinic. During our walk through the mall after a tour of the new clinic – we are greeted by two of his former patients who are pleased to see him. One young lady ruefully shrugs with a shy smile while showing off her advanced pregnancy, as if acknowledging that she will be back soon.
Hopefully, we will follow Dr. Botero to the operating soon.
After spending some time in my old neighborhood in Bogotá visiting friends and family over the holiday weekend – it was time for a quick trip to Barranquilla for another reunion, of sorts. Dr. Hector Pulido, the Chief of Surgery at the Clinica General del Norte (and a long-time friend) invited me to Barranquilla to take a look around..
with Dr. Hector Pulido (left) and Dr. Barbosa in Cartagena (2010).
The City of Barranquilla: Colombia’s Golden Gate
Barranquilla is the capital of the Colombian state (province) of Atlantico, and is the largest city within Atlantico. Barranquilla is the fourth largest city within Colombia – after Bogotá, Medellin and Cali. While population estimates vary greatly, the generally published estimate is around 1.6 to 2.4 million people*. Much of Barranquilla’s historical importance is related to its position as the major port of Colombia. This is reflected in Barranquilla’s continued growth and reputation today.
Barranquilla: More than Shakira and Carnival
While Barranquilla is widely considered to be Cartagena’s ugly big sister; it is also the coastal region’s more serious, intellectual and industrial side. Excluding the internationally famous Carnival; among the Colombian coastal cities of Barranquilla, Cartagena and Santa Marta; Cartagena is viewed as being for play, Santa Marta for relaxation… But Barranquilla is viewed as the city where the work gets done..
That impression; of business-like efficiency and competency certainly held true during my tour of the main facility of the rapidly expanding Clinica General del Norte health system.
Clinica General del Norte
The Clinica General del Norte facility on Calle 70 is the main facility of the nine hospital network. (There are 4 hospitals in Barranquilla itself, with several other hospitals in Cartagena and other coastal areas.) The Calle 70 facility is also the biggest with 464 beds, and an anticipated addition of 300 beds in the works.
Care of the critically ill
Clinica General del Norte has 100 intensive care beds, with a dedicated coronary /cardiac intensive care, a burn unit, pediatric intensive care and a 24 bed neo-natal unit. They also have an intensive care unit for patients requiring hepatic dialysis for patients with liver failure. This last unit is of particular interest – since it is where Dr. Hector Pulido, as a general surgeon specializing in Liver, Biliary, Pancreatic Surgery and Transplant) cares for many of his more critically ill patients after surgery.
But no real chance to observe Dr. Pulido at work – at least, not today.. Just a quick whirl around the facility, accompanied by Yolanda Basto de Hossman, and Dra. Maria del Carmen – to the 14 operating rooms to check out the cardiac surgery room along with the updated and modern equipment, to the neo-natal unit to talk to the Chief of Pediatrics, and see babies as young as 20 weeks gestation.
MRI/ CT scan and Angiography facilities
Dr. Pulido encourages them to show me everything (everything! he says) – so they do; the dual angiography suites, the 64 slice CT scanner with 3D reconstruction, to MRI – meeting and talking to staff along the way. No PET/ CT yet but it’s on the way – they say – which will make this the only facility on the coast with such diagnostic capabilities. (They are building the structure to contain it as part of the new building being constructed in front of the existing facility).
But, of course, for me – it’s not enough.. I need to talk to the surgeons, spend some time with them; observing and talking to their patients – getting the feel and the rhythm of their practice.. I need to watch them in the operating room, and to know them – before I can be completely satisfied.
So even now, as Victor takes me back to the airport, I am thinking, questioning, planning.. “Are the rents very expensive near here?”, I ask. “No” he says as he drives through the nearby small streets with gaily painted houses.. Well, then I think I have my answer.
Sunset in on the air field as I prepare to leave Barranquilla
Clara and her family have a special place in my heart. I first met them when I rented an apartment from them for almost six months while researching the Bogota back. I have been back several times since, and I always stay with the Palacios.. They are wonderful people who typify the kind and generous nature of Colombians in general.
The other day, while at the fruit market, I purchased several Brevas. Despite all of my previous visits – I remained fairly ignorant of this particular Colombian fruit, which is a type of fig.
Mangostinos and brevas. Brevas are the small green fruit
So, Clara was kind enough to share a recipe for making a desert of Brevas that has been in her family for over 100 years, which I will now share with you. As a spectacularly bad cook – I was smart enough not to get too close as we were cooking, but I took copious notes. (When I cook, the fire department is often involved.)
The recipe is fairly simple – simple enough that I can probably manage myself next time. The ingredient list includes: Brevas, washed and rinsed, about a half cup of sugar (or panela) and cinnamon.
panela
1. After rinsing the brevas, cut of the ends. Then partually section each breva. (Do not cut into pieces, just make a small cut at the top of the breva, extending about half way down the fruit).
2. Place in a saucepan, and cover with water.
3. Add about 1/3 to 1/2 cup of sugar (or panela) to the mixture.. and 1/2 tsp of cinnamon (or one small stick of cinnamon broken into smaller pieces)
4. Boil until the mixture thickens to a syrupy glaze (about 20 – 25 minutes.) This mixture will be dark brown (from the cinnamon).
Boiling brevas: Photo by Camila
5. Serve warm with a slice of mild cheese (queso de crema).
Traditionally served with a mild white cheese and cold milk
Delicious! The cheese is a perfect contrast to the sweet rich taste of the brevas..
I am visiting Bogotá this week, before heading back to Medellin..
Bogotá is one of those cities that climbs into your heart – despite initial misgivings; too big, too cold, often rainy; becomes gloriously interesting and wonderfully cool..
I was armed with just a camera phone, so my friend, Camila Togni assisted in my photo-taking endeavors..
Sidewalk in downtown Bogota
Despite its large size – the city manages to be hospitable and friendly to visitors – and I missed my Bogotá “home”. So I headed back for just a few days to check in and enjoy all the things that make me love this unlikely city so much..
While Barrio Chico (where I live) is pretty quiet – La Candelaria is always quite a bit more lively.
I normally tend to avoid the Candelaria area because of the ever-present crowds of people, which is a shame because there are a lot of interesting places to visit and some beautiful architecture in this part of town.
Alvaro Palacio & Claro Lozano in front of the Cathedral de Bogota
But this weekend is the celebration por el nino del 20 de julio (and the ORs are closed) so when my friends invited me to go downtown with them – it was an opportunity not to be missed!
First we headed to the Iglesia de nino de 20 de Julio since this what the holiday weekend was all about.. It’s a huge church – a campus, actually – and it was packed with people.
Iglesia de nino del 20 de Julio
Even though it was crowded, it was a lovely service – and the church itself is quite pretty.
el nino de 20 de Julio
The church has a lovely glass dome and several stained-glass windows with religious scenes.
The church is so large, the domed area actually isn’t part of the central church, but an overflow area with a jumbo screen television so worshippers can see the priest conducting the service in the main chamber.
You can see the crowd milling in the foreground of this photo.
the crowd at the church
After the service, we wandered around the large flea market just a street away from the church before heading to lunch at a famous but tiny, and old restaurant called, “La Puerto Falso.”
While the rest of my party had their famous tamals, I was up for a bit of a culinary adventure, so I had a soup called Changua.
Colombian Tamal
While the description of a soup made of milk, eggs, bread, mild local cheese and cilantro didn’t sound that entices – it was actually quite good and is part of Bogotá regional cuisine.
Links for additional information about sightseeing in Bogota
Most guides are going to send you to the Museo de Oro “The Gold Museum” but that’s not my favorite..
Museo de la Policia – probably my favorite of all the museums, thus far, in Colombia. It’s free – guides welcome you in from the street – and you can see the bloodied, bullet-ridden jacket of Pablo Escobar, from his last moments on a rooftop in Medellin. (It’s considered rude to ask about Pablo Escobar in general conversation) but if you hold any fascination about how a rural boy from an impoverished background managed to hold Colombia hostage, and gain international infamy – it’s a must. The guides also offered free candy, and played a game of ‘rana’ with us. (The are guides for multiple languages).
the crowd at the Botanical Gardens enjoys a free show during the International Tango Festival
While salsa dancing is a Colombian original (from Cali), the Argentine tango is alive and well here in Medellin. At this week’s festival, several musicians and dancers from Medellin are being showcased for their skills – along with Buenos Aires legends.. Local schoolchildren are also participating in a series of concerts and dance demonstrations. It’s quite a bit of fun – and showcases some of the things the city of Medellin really excels at.
After attending a Tango performance last weekend, and numerous other public events and outings – one of the things that it really noticeable is how well the city manages these events.
Fun and family friendly
There has been no trash or litter, no displays of public drunkenness (despite the fact that there is plenty of alcohol at these events), and no disturbances at any of our outings (and several were free).
Roaming the city
During the weekend, we roam the city – taking pictures, enjoying the endlessly lovely weather – and riding on the metro (train). The trains are affordable, quick (and if you avoid peak traveling times during the week) not too overly crowded.
above ground metro train
Universidad Station
Several parks and museums are located close to the Universidad Station including the Planetarium, Parque Explora (for kids) and the Botanical Gardens.
the planetarium
The Botanical Gardens
The ‘Joaquin Antonio Uribe’ Botanical Gardens were a delightfully relaxing place to spend a gorgeously sunny Sunday afternoon in the midst of the city, but away from the hustle and bustle of El Centro (where I live).
Admission is free.
There was live music to listen to, plenty of flowers, and wildlife to enjoy (iguanas roam the grounds), and assortment of snacks (ice cream, juice drinks, and other regional treats).
Iguanas roam the park
But the park isn’t just there to enjoy nature.. It’s a great place to people watch.. Also the people of Medellin are very kind and friendly, so they are happy to talk – even to gringas with bad Spanish, like myself.
using his camera to meet girls
We watched this photographer use his camera to meet girls as he roamed the park..
A group of young people singing…
Then we met a lovely princess..
and a local vendor selling gum in the park..
lost his leg due to a landmine
This very nice gentleman is a reminder that as sunny and lovely as Medellin is – there is still an ongoing war to remember.. One that has devastated thousands of young men, and displaced millions of people.
jumping rope
Wholesome
As a visitor (and temporary resident) of Medellin – the wholesomeness of the park is enchanting.. It’s a reminder of one of the reasons, I do enjoy Colombia so very much.. Just like my “Sundays in Bogotá” – the city slows down during the weekends, and people spent time with their loved ones.. No gameboys in evidence, and phones used mainly to take pictures.. It’s a gracious illusion that reminds me of my own childhood in a small town..
I apologize for the wordiness of this post – but much of what we discuss below is covered in the Bogotá, Cartagena and Mexicali books – the essential mechanisms of cardiac surgery; how procedures work, what is off-pump surgery, when do we use the bypass pump and other explanatory information. But since I have am not writing a full book on Medellin, I wanted to offer a bit of a primer for my new internet readers here.
Dr. Luis Meza
Cardiac surgeon, Hospital General de Medellin
After interviewing Dr. Meza and meeting many of the staff at Hospital General de Medellin, it was a pleasure to be invited to observe Dr. Meza and Dr. Urequi , the head of the cardiac surgery department in the operating room. Despite the patient’s young age, the surgery (for me as an observer) was knuckle-biting. While the surgery itself was a fast, straight-forward and uncomplicated repair of an interauricular septal defect – it was the patient’s fragile condition that had me on the edge of my seat.
Complex patients The case was typical of many of the cases they see at public hospitals. It was a young patient with newly diagnosed right-sided heart failure due to an uncorrected congenital defect. The patient had traveled from another part of Colombia (one of the poorer regions) to have surgery. The patient had initially presented to a local doctor after a syncopal event (passing out) and was found to have an enlarged heart, with a moderate sized pericardial effusion (fluid in the sac around the heart.) After arriving at HGM, the patient was also diagnosed with a serious acquired coagulopathy (bleeding disorder).
drawing courtesy of Wikipedia (Creative Commons licensing)
Since the patient had a hole between the left atrium leading into the right atrium, blood was being pushed from the left atrium (which is under higher pressure) to the low pressure right atrium. Over the course of many years, this had caused the right atrium to enlarge massively. As the right atrium was continuously being overfilled (from blood from the left side), the right side of the heart was being forced to work harder, and harder. As the atrium continued to be overstretched, and enlarged – it also caused blood to be forced back into the pulmonary arteries – causing pulmonary hypertension. While pre-surgical tests (echocardiogram, and cardiac catheterization) showed the patient to have (only) moderate pulmonary hypertension (with PA systolic pressures of 65mmHg).
Pre-operative testing is only part of the story
However, when we looked down, into the patient’s chest – it was obvious that the patient’s pulmonary vasculature was engorged and enlarged. The patient’s heart was massive, and floppy (which is a sign the heart is working way too hard). The patient also had peripheral edema which is another sign that the heart was not working well.
Potential for badness*
So even though, the surgery itself (described below) is not terribly technically challenging (‘like darning socks’ one surgeon used to say) – a lot can go wrong because the patient’s heart just doesn’t work that well to begin with.
* a not-so-scientific term to describe the likelihood of potential complications, problems or adverse outcomes. These may be unavoidable circumstances in many cases – but the term is a reminder to remain vigilant even during so-called “simple” procedures.
Nitric oxide on hand
This OR does have nitric oxide – (which we didn’t need), but was available nearby, just in case. Nitric oxide, milrinone and other medications are critical to have on hand in patients with pulmonary hypertension. Some patients will never need it – others can’t survive without it – and sadly, (in patients with severe fixed pulmonary hypertension), nothing – not even an assist device is going to make much difference. While we can try to predict which patients are going to tolerate surgery, it’s not always clear-cut. Tests (echocardiograms, right heart caths) can predict, tests can give probabilities – but sometimes tests are wrong, and patients who appear to have only ‘mild’ disease do very poorly (and visa versa). Sometimes, we just have to hold our breath as the patient comes off bypass and see.
canisters of nitric oxide in OR #1
As I mentioned in a previous post – cardiac surgery procedures can be a bit more complicated than many other surgical procedures, and while having something like nitric oxide on hand doesn’t seem like a big deal – it is. (I have worked in several facilities without these capabilities). It also speaks to the general preparedness of the staff. But despite the ‘potential for badness’ everything proceeded beautifully with Drs. Urequi and Meza. The case seemed to speed by despite the patient’s fragile health. The entire CPB (cardiopulmonary bypass run) was just 26 minutes with a total cross-clamp time of 31 minutes.)
A little bit about cardiopulmonary bypass – the “heart-lung machine”
In comparison to the congenital repair above, average CPB times for valve replacement run around 100 minutes, 60 to 90 minutes for bypass surgery. Patients have a higher risk of CPB related complications from hypo/ altered perfusion after long pump runs . As the clock begins to exceed 120 minutes, the risk of renal failure, cognitive changes and bleeding problems (as blood cells are continuous smashed/ broken / damaged within the pump) increase.
What is “Off-pump surgery”? Nowadays, lots of people get real excited about “off-pump” surgery because they think that by not using the heart-lung machine, they can avoid a lot of the problems we mentioned above. But that’s oversimplifying the entire scenario – and one that I find is often used to “sell” a particular surgeon or surgical program. Off-pump can be safer than CPB cases, for some patients. But these are usually not the patients that the surgery is sold to.. So it’s important to know what some of the terminology really means. Just because Hospital X has billboards announcing that they now perform off pump surgery – doesn’t mean that it’s something you may even need or want.
Off pump is not for everyone
Patients have to be fairly healthy to tolerate cardiac surgery without the pump. People with a lot of the problems that we thought were worsened by the pump, actually fare worse when we try to do surgery without the heart-lung machine. For example, we initially thought that Off-pump surgery would be great for people with renal insufficiency or ‘bad kidneys’ – particularly people who have kidney problems but aren’t quite sick enough to be on dialysis yet. The hope was that by avoiding the bypass pump we could avoid any damage to the kidneys from artificial flow/hypoperfusion because one of the biggest risks of cardiac surgery in patients with bad kidneys is that surgery will cause their kidneys to fail entirely, and make patients dialysis dependent. Unfortunately, the research from all of the off-pump surgeries being done hasn’t really shown the benefits that we thought it would. So like most things in medicine, it’s not quite the panacea we had hoped it was. But we did learn an incredible amount of information once surgeons started trying off pump surgeries for coronary bypass. Surprisingly, we learned that many of the complications, and conditions that we had long blamed on the CPB pump – weren’t related to the machine at all. But much of this is still being argued by cardiac surgeons every single day – each with different research studies giving different results..
More importantly, Off-pump not possible for many types of cardiac surgery
It’s technically impossible to do some types of cases without the bypass pump. Coronary bypass surgery (CABG) is very different from other types of surgery, for example. During bypass, the surgeon is only operating on the outside of the heart – attaching new conduit (arteries and veins) to arteries on the surface of the heart. So – it isn’t absolutely essential to have the pump circulating blood for him while he’s operating – in some patients – we can let their body do it for us during surgery.
But replacing diseased heart valves, or the great vessels (aortic aneurysms etc) is a completely different entity. In those surgeries – the surgeon is cutting into the heart or great vessels themselves. It’s not possible to lop off the top of the aorta, operate on the aortic valve and not have blood being re-directed mechanically during this process. Otherwise blood would just literally spill out into the chest and never oxygenate the brain and the rest of the body. (The only time we ever do this kind of procedure without a pump is during organ retrieval – for obvious reasons). It’s important to know these distinctions so people understand how the surgery actually proceeds.
For the case today – the surgeon has to make an incision through the side of the atria (wall of the heart chamber) to get to the hole on the inside wall of the heart.) The surgeon then closes the hole with suture (and a patch, in some cases). Some doctors do this in the cath lab without surgery – but that’s also controversal because the patch used in the cath procedures in the past has caused a high incidence of stroke. In a young patient like the one here – you certainly wouldn’t want to risk it – particularly since we don’t know how well those patches hold up in the long term.
Cardiac surgeons operate at Hospital General de Medellin (HGM)
Overall evaluation of today’s case:
Safety checklists, and all pre-operative procedures were completed. Patient was prepped and draped in an appropriate sterile fashion. Antibiotics were administered within the recommended window (of time). Appropriate records were maintained during the case.
Surgery proceeded normally and without incident.
Due to an underlying coagulopathy the patient did require administration of nonautologous blood products (4 units of packed red blood cells, 3 packets of platelets, and abumin) while on pump. While the facility does not have a ‘cell-saver’ for washing and re-infusing shed blood, patient did receive autologous(their own) transfusion from the CPB pump. This blood, from the CPB circuit was returned to the patient to limit the amount of blood needed after surgery. Hemoglobin at the conclusion of surgery was 9.6mg/dl, which is within acceptable parameters.
Hemostasis was obtained prior to chest closure, with only a small amount of chest tube drainage in the collection chamber at the time of transfer to the intensive care unit.
Surgical Apgars – do not apply for cardiac cases due to the nature of the case, and use of CPB. Mean pressure while on CPB was within an acceptable range. Patient’s urinary output was less than anticipated during the case (150cc) despite the use of mannitol while on pump, but the patient responded well (1000+) with volume infusion and the addition of furosemide.
The patient was hemodynamically stable during the entire case. The was a very brief transitory period of hypotension (less than 5 minutes) near the conclusion of the case, which was immediately noted by anesthesia and treated with no recurrence.
On transfer to the unit, the patient was accompanied by several members of the OR staff, including Dr. Meza, the anesthesiologist, and the perfusionist, each of which did a face-to-face “hand-off” report of the patient (and medical history) including the course of the surgical procedure (including medications given, lab values, procedural details) to the Intensivist (physician), with ICU nursing staff attending to the patient.
Transesophageal echo (TEE) was not performed during this case, but was available if needed.
Also, I am happy to report there were no smartphones or “facebooking” in sight. No one appeared engaged in anything other than the surgery at hand.
If you’ve never been to the cardiac operating room – it’s a completely different world, and not what most people expect. For starters, unlike many areas of health care (particularly in the USA), the cardiac operating room is usually very well staffed.
Just a few of the people working in the OR. (photo edited to preserve patient privacy)
For example, there were eight people working in the operating room today:
Dr. Suarez observes her patient during surgery. (photo edited to preserve patient’s privacy)
Ms. Catherine Cardona, “Jefe”/ Nurse who supervises the operating room
Ms. Diana Isobel Lopez, Perfusionist (In Colombia, all perfusionists have an undergraduate degree in nursing, before obtaining a postgraduate degree in Perfusion). The perfusionist is the person who ‘runs’ the cardiac bypass machine.
Ms. Laura Garcia, Instrumentadora (First Assist)
Angel, circulating nurse
Olga, another instrumentadora, who is training to work in the cardiac OR.
This is fairly typical for most institutions.
Secondly – it’s always a regimented, and checklist kind of place. (I wish I could say that about every operating room – but it just wouldn’t be true.) But cardiac ORs (without exception) always follow a very strict set of accounting procedures..
For starters – there are labels.. For the patient (arm bands), for the equipment (medications, blood products etc..) even the room is labeled.
Sign on operating room door (edited for patient privacy)
Then come the checklists..
Perfusionist Diana Lopez gathers information to begin her pre-operative checklist.
The general (WHO) operating room checklist. The perfusionist’s checklist.. The anesthesiologist’s checklist.. and the big white cardiac checklist.
by the end of the case, this board will be full..
The staff attempts to anticipate every possible need and have it on hand ahead of time. Whether it’s nitric oxide, blood, defibrillation equipment, or special medications – it’s already stocked and ready before the patient is ever wheeled in.
Most of these things are universal:
such as the principles of asepsis (preventing infection), patient safety and preventing intra-operative errors – no matter what hospital or country you are visiting (and when it comes to surgery – that’s the way it should be.)
Today was no exception..
In health care, we talk about “OR people” and “ER people”.. ER people are the MacGyvers of the world – people who thrive on adrenaline, excitement and the unexpected. They are at their best when a tractor-trailer skids into a gas station, ignites and sets of a five-alarm fire that decimates a kindergarden, sending screaming children racing into the streets.. And God love them for having that talent..
But the OR.. that’s my personal area of tranquility.
This orderly, prepared environments is one of the reasons I love what I do.. (I am not a screaming, “by the seat-of-your-pants”/ ‘skin of your teeth’ kind of gal). I don’t want to encounter surprises when it comes to my patient’s health – and I never ever want to be caught unprepared. That’s not to say that I can’t handle an emergent cardiac patient crashing in the cath lab – it just means I’ve considered the scenarios before, (and have a couple of tricks up my sleeve) to make sure my patient is well taken care of (and expedite the process).
That logical, critical-thinking component of my personality is one of the reasons I am able to provide valuable and objective information when visiting hospitals and surgeons like Dr. Urequi’s and Dr. Meza’s operating room at Hospital General de Medellin.
In OR #1 – cardiothoracic suite
As I mentioned in a previous post on Hospital General de Medellin, operating room suite #1 has been designated for cardiac and thoracic surgeries. This works out well since the operating room itself, is modern and spacious (which is important because of the area needed when adding specialized cardiac surgery equipment like the CPB pump (aka heart-lung machine). There are muliple monitors, which is important for the video-assisted thoracoscopy (VATS) thoracic cases but also helpful for the cardiac cases. The surgeon is able to project the case as he’s performing it on a spare monitor, which allows everyone involved to see what’s going on during the case (and anticipate what he will need next) without shouting or crowding the operating room table.
Coordinating care by watching surgery
For instance, if the circulator looks up at the monitor and sees he is finishing (the bypasses for example), she can make sure both the instrumentadora and the anesthesiologist have the paddles and cables ready to gently defibrillate the heart if it needs a little ‘jump start’ back into normal rhythm..or collect lab samples, or double check medications, blood products or whatever else is needed at specific points during the surgery.
As Colombia’s profile continues to rise as a medical tourism destination, Proexport is launching a new campaign which will air on international media such as the Discovery Health channel. As reported in the Curacao Chronicle, Colombia is becoming a destination of choice for high complexity medical procedures, and expanding to include visitors from a myriad of destinations, including North America.
Historically, patients from the Caribbean have come to Colombia for medical tourism due to the lack of even basic services in most Caribbean nations – which is something travelers should keep in mind now that Barbados, and several other islands have launched their own medical tourism campaigns.
The growing role of Planet Hospital in Colombia
The only alarming part – appears to be the heavy participation of Planet Hospital in the world marketing of Colombian medical services. Planet Hospital, a massively successful medical tourism company, which proudly exists in a ‘no mans’ land” of ethics (according to founder, Rudy Rupak). The company also prides itself on its global forays into surrogacy and transplant tourism, both of which are highly controversal.
Selling babies… and organs
While people can continue to argue the ethics of the surrogacy baby trade, the murder of Chinese and other citizens for organ transplantation should give anyone pause. Or the fact, that companies like Planet Hospital will send potential patients to someone who isn’t even trained in transplant…
But that hasn’t stopped Planet Hospital in their quest, the ever-expanding global tourism empire has seemingly become more bulletproof in the last few months. Multiple websites, blogs and news articles that detailed corruption and casualities (as well as problems behind the scenes) at Planet Hospital have seemingly disappeared.
Now it appears Planet Hospital will be adding Colombia to it’s stables and laughing all the way to the bank.
Dr. Luis Fernando Meza Valencia, cardiac surgeon and his wife, Dra. Elaine Suarez Gomez, anesthesiologist have a terrific partnership as part of the Cardiac Surgery program at Hospital General de Medellin (HGM). (Hospital General de Medellin is one of just a few public hospitals that have heart surgery programs.)
Dr. Meza, a Cali native who trained at Fundacion Cardioinfantil under the instruction of Dr. Pablo Umana, Dr. Nestor Sandoval along with Dr. Maldonado now performs coronary bypass, valve replacement, surgery on the great vessels (such as ascending arch replacement, aortic aneurysm repair) at the Hospital General de Medellin as well as several smaller, private facilities like Clinica Las Vegas.
He has worked at HGM for 2 1/2 years since he moved from the public hospital in Manizales (in the coffee-growing region of central Colombia).
Dra. Elaine Suarez is a anesthesiologist who has specializes in cardiothoracic anesthesia. She has been practicing for five years and is fluent in English and German in addition to her native Spanish.
High risk patients
Because HGM serves the public and many of their patients are impoverished, Dr. Meza and Dra. Suarez see a large number of rheumatic heart disease and endocarditis patients. Many of these patients have had very limited preventative care or medical management of their underlying chronic health conditions. A large number of these patients have significant co-morbid conditions such as diabetes, chroic pulmonary disease, hypertension, hyperlipidemia, and nephropathies (kidney damage). This subset of patients almost always presents in the midst of a cardiac emergency.
In the Consulta Externa
Dr. Meza reports that he usually spends at least an hour with his patients during the initial consultation, gathering information, examining the patient and explaining the necessary tests and treatments.
In the Operating Room
Haven’t had an opportunity to follow Dr. Meza to the operating room yet, but we did get to see Dra. Suarez in action.
I am still working on several posts – but in the meantime, I wanted to post some photos from my visit to the operating room with Dr. Wilfredy Castaño Ruiz, one of the thoracic surgeons at Hospital General de Medellin.
Readers may notice that some of the content of my observations of the operating room have changed.. In reality, the reports haven’t changed – I have just chosen to share more of the information that I usually reserve for the books since I probably won’t get time for a “Medellin book”. So, if you are squeamish, or if you don’t want to know – quit reading right about now…
It was a surprise to meet Dr. Wilfredy Castaño Ruiz because it turns out we’ve already met. He was one of the fellows I encountered during one of my early interviews in Bogota, with Dr. Juan Carlos Garzon Ramirez at Fundacion Cardioinfantil.
Since then (which was actually back in the early spring of 2011), Dr. Castaño has completed his fellowship and come to Medellin.
Dr. Wilfredy Castaño Ruiz, thoracic surgeon at Hospital General de Medellin
Yesterday, I joined him in the operating room to observe a VATS decortication. The case went beautifully.
Dra. Elaine Suarez Gomez, an anesthesiologist who specializes in cardiothoracic anesthesia managed the patient’s anesthesia during the case. (This is important because anesthesia is more complicated in thoracic surgery because of such factors as double lumen intubation and selective uni-lung ventilation during surgery).
Anesthesia was well-managed during the case, with continuous hemodynamic monitoring. There was no hypotension (low blood pressure) during the case, or hemodynamic instability. Pulse oxymetry was maintained at 98% or above for the entire case. Surgical Apgar: 8 (due to blood loss**)
Monitors at HGM are large and easily seen from all areas of the OR
Dr. Wilfredy Castaño Ruiz was assisted by Luz Marcela Echaverria Cifuentes, (RN, first assist*). The circulating nurse was a very nice fellow named Mauricio Lotero Lopez.
Enf. Luz Echaverria assists Dr. Wilfredy Castaño Ruiz during surgery.
*”Registered nurse” is not terminology common to Colombia, but this is the equivalent position in Colombia, which requires about six years of training.)
** In this particular case, the surgical apgar of 8 is misleading. The anesthesia was excellent, and the surgery proceeded very well. However, due to the nature of surgical decortication (for a loculated pleural effusion/ empyema) there is always some bleeding as the thick, infected material is pulled from the lung’s surface. This bleeding was not excessive for this type of surgery, nor was it life-threatening in nature.
I spent the day yesterday at Hospital General de Medellin, and I am going back today for another visit. I’ll be revising and updating this post as I go along. I spend most of the day with Dr. Luis Fernando Meza Valencia and Dra. Elaine Suarez Gomez, but we will talk more about these two doctors in another post.
Quite frankly, it is the nicest public facility I have ever been in, anywhere. The entire facility (and I was peeking in corners and closets) was spotless – and that included the operating rooms.
It’s the main trauma center for Medellin, and the largest public facility with a large well-coordinated ER. (The ER was quiet and orderly during my visit – despite being about half-full.
The hospital is well-equipped with 3 mixed ICUs, a step-down unit, a large neonatal ward and NICU, pediatric ICU along with multiple wards for medical patients. There are nine operating rooms, including a dedicated cardiac operating room (quirofano #1), and a separate cath lab with OR capabilities (for endovascular and hybrid procedures.)
Attached to the hospital is the ‘Consulta Externa’ where the doctors see their patients, along with a non-invasive cardiology clinic (echocardiograms, stress tests and the like, and laboratory. I have certainly missed several departments – as I passed auditoriums and several other departments during my visit, but all of the major elements are included above.
They do not have a PET scanner at Hospital General de Medellin (but given the expense of this machinery, there are only a few PET scanners in Colombia. There are only two in Bogotá – one at the Fundacion Santa Fe de Bogotá, and one at the National Cancer Institute.)
There is no international patient division or department, but the website has a full English version, many of the physicians speak English (about half of the physicians I met), and they are very welcoming.
Mural at Hospital General de Medellin
The hospital, while busy was not as hectic or crowded as some of the other facilities I have seen in the past. I’ll be at Hospital General for multiple visits, so I will have plenty of opportunities to see if that changes.
High-risk Obstetrics Program
During my visit – Dr. Carlos Garcia, the Chief of Surgery was talking about the new obstetrics outpatient monitoring program along with several other services that are fairly uncommon for publicly funded hospital facilities.
I only received the basics of the OB program (because OB is not really my area of expertise) but as Dr. Garcia explained – it’s an out-patient monitoring program for high-risk obstetrics patients. Patients are equipped with fetal monitors so that they can be in their own homes during much of their gestational period, instead of confined to the hospital. The monitors are reviewed continuously by the staff at Hospital General – and if there are any serious abnormalities or evidence of fetal distress, not only is the patient contacted – but an ambulance is automatically sent to bring in the patient for urgent/ emergent evaluation and treatment.
I was hoping to collect information on surgeons and surgery here in Medellin for publication in a series of articles as well as a potential collection(another book, perhaps) but so far – the surgeons of Medellin have proven to be quite elusive to my attempts to contact them.
Hopefully my luck will change, so I am able to bring all of you news about what’s new, innovative, or simply outstanding in medicine here in Medellin..
I don’t know how it always happens.. I set out on one kind of expedition and (frequently) it turns into something else. So we have it.. I was planning to write extensively on Panama City, but looky, looky – here I am again, living in the fantastic, tragic beauty of Medellin.
As I wrote once before, Medellin is a city of great loveliness, but somehow Bogotá always blinded me to Medellin’s charms.. But it’s time to give Medellin a fair shake, so here I am..
It’s not his first visit – he’s done several other programs highlighting Colombia, but tonight’s episode on his new CNN show, “Parts Unknown” is definitely his best. It’s the first time I think he actually ‘got it’ and was really able to convey a real sense of Colombia to his viewers.
While his previous shows were primarily about food, and local food culture – his episodes on Colombian cuisine were always very wide from the mark.. Sure, he had the names of dishes and such – but he didn’t really bring home the feel of Colombia and it’s people.
Or that Colombian food isn’t really about intense spices, it’s about the intense and rich flavors that comes from the rich textures of the foods themselves – without overpowering curries or heavy sauces..
Better quality, fresher ingredients and a wide variety make for richer flavors
Was it a medical mistake/ an accident of fate / or…. was it the Cocaine? An inquest is held on the intra-operative death of an Irish medical tourist..
In a recent inquest, the wife of an Irish tourist who died while undergoing liposuction with a well-known Colombian plastic surgeon talked about her husband and his decision to pursue plastic surgery with Dr. Ricardo Lancheros Pedraza.
In a published story by Gareth Naughton of the Irish Independent, the wife of Pierre Christian Lawlor detailed her husband’s decision to undergo cosmetic surgery with the Bogotá surgeon due to unhappiness with his physique.
During her testimony, she also conceded that her husband had taken cocaine in the days and hours immediately prior to surgery – despite being advised specifically to refrain from smoking, alcohol or taking medications.
In a story published in Irish Central – Ms. Andrea Galeano, the Venezuelan-borne wife of Mr. Farrell reported that her husband had taken cocaine on several occasions after arriving in Bogotá for his surgical procedure.
Mr. Farrell is believed to have died from intra-operative myocardial infarction (heart attack during surgery).
Additional Information
This Daily Mail article from 2012 describes how the use of cocaine can cause heart attacks, and sudden cardiac death.
While I am back here in the United States, I wanted to share many of the images I’ve gathered and collected during my most recent visit to Colombia.. Some of these images will be familiar to long-term readers from various posts about my trips to Lerida, visits to the finca, and day-to-day encounters with different and interesting people in Colombia.
I hope you enjoy!
People and Places in the nation of Colombia
on a Techo por mi pais building project – in south Bogota
on a Techo por mi pais building project – in south Bogota
on a Techo por mi pais building project – in south Bogota
on a Techo por mi pais building project – in south Bogota
students from the local beauty school, south Bogota
everything gets recycled – these panels are used for roofing
kids playing in South Bogota
Techo family
the finished house
the best model for a novice photographer..
Jo
a ranch hand at a working finca outside Bogota
My friend, the photographer, documenting Colombian life
sunset in the mountains above Bogota
one of my favorite models – at a finca
a view of Bogota at night
vacation finca
buying fruit at the side of the road
ruins of Armero, site of volcano tragedy
a vacation finca
in Lerida
street in Lerida
ruins at Armero
in Tolima
training school for police pilots
Church in Mariquita
the bogota castle
Not what I was expecting
working on the mural
Bogota mural artist
Bogota cityscape
a work in progress
a homeless woman rests against a construction barrier of one of the newest Bogota high rises
The Hotel B3 on Carrera 15
lazy Sunday in Usaquen
Usaquen
vintage rides in Usaquen
A girl offering puppies in the park (with parents, not pictured)
German Encino and his wife at one of my favorite casual restaurants
As my long-time readers know – I am a huge fan of Adriaan Alsema, a Dutch-borne journalist in Medellin, Colombia. He is the founder/ creator/ and genius behind Colombia Reports.com – the English language news source for all things Colombiano.
Much thanks to Jose Vergara for sending me a link to an article on Dr. Alejandro Jadad. Jose Vergara, aka Frankie Jazz, as some readers may remember, is a Cartagena native and talented artist in his own right.
Frankie Jazz/ Jose Vergara
We try to keep up with each other – so he knows all about my interest in Colombian medicine and surgery, and I love his new album (so I try not to gush and be too much of a groupie when I hear from him) but he recently sent me a link to one of his more recent projects. The Voxxi article by Silvia Casablanca is pretty interesting, so I wanted to share it with readers.
For starters – Jose Vergara is the photographer for the article..
Dr. Alejandro Jadad, MD, PhD
But it’s the life of Dr. Alejandro Jadadthat is so inspiring.. Dr. Jadad is a Colombian anesthesiologist, textbook author and founder of the Centre for Global eHealth Innovation in Toronto, Canada (among other things). He has been credited with being one of the major innovators in the fields of clinical research, medicine and information technology.
While at Oxford, as a research fellow in Anesthesiology, he developed a validation tool (the Jadad scale) to critically evaluate and analyze clinical research studies. This is an important tool to distinguish the quality (and value) of individual research studies – or how much weight a study (and its findings) should have. We talk about the importance of objective scales and measures quite a bit here at Bogotá Surgery, and the Jadad scale is one of the best known and most widely used scales for clinical research.
Clinical research is how surgeons know whether a patient has a better chance for survival with surgery or chemotherapy/ radiation, for example.
So as you can imagine – having a tool like this is particularly vital when talking about clinical medicine / or health research where the findings of research studies are used to guide and determine medical decisions – aka the medical treatments for people like in our example above.
As the Casablanca article points out – Dr. Jadad didn’t stop with writing textbooks and creating the Jadad scale. After completing his fellowship in the United Kingdom, he moved to Ontario, Canada to continue his research at McMaster University. Since then, he has continued to innovate and create tools to help both clinicians and the public. One of the ways he helps clinicians is by further creating and refining tools to evaluate medical research.
He has also been a major creator and contributor to the development of internet and computer based applications to connect doctors and their patients. His efforts are based on more that the patient – provider dyad, and are part of a larger, global framework for reforming and transforming healthcare.
Just a week ago, I was ankle-deep in mud in the southern-most reaches of Bogotá, with ‘Team Sanabria’ as they completed another house as part of “Techo por mi pais”, which is an organization very similar to Habitat for Humanity.
A couple of weekends each year, they donate their time (and hard labor) to build homes for many of Bogotá’s poorest residents.
It’s arduous work – which is more difficult given the frequent rain and adverse weather conditions in the hills above Bogotá.
I wrote a short story about their efforts over at Examiner.com – but I wasn’t able to include all of the pictures, so I wanted to post some of them here.
Juan Jesus’ grandson stands in the doorway of his modest home
The family they were building the house for on this occasion was exceedingly sweet, gracious – and willing to wade into the muck with the rest of the team.
The organization, is much bigger than just Team Sanabria, so all in all – about fifty houses were built that weekend.
Volunteers carrying supplies to another site
laying foundation for Juan Jesus’ new house
It costs about 1500 dollars to construct one of the basic 3 meter X 6 meter homes.
Here the foundation, and flooring has been completed – and they are getting the walls into place.
Luckily, the rain didn’t start again until most of the walls were completed.
It was an excellent chance to see a side of Bogota that most visitors never to get see – and to meet many of the residents of the neighborhood, so I was very glad they invited me to join them.
a group of beauty school students stop by to check on the progress.
It also gave me a chance to get some other pictures of the neighborhood – of things we don’t often think about when we see or hear about poorer neighborhoods (or slums).
Like the rose bushes that residents plant to brighten and beautify their homes.
well kept home with flowers
Or the full herb garden, Juan Jesus’ neighbor planted (and shared with us) in her immaculately kept and fenced yard.
I think sometimes, the overwhelming poverty makes it hard for outsiders to notice the little spots of beauty in places like this. But it gives me hope – and it shows the resilience of human nature.
I think it’s also important right now, while our own country is hurting too.. With all of the divisions and politics – particularly in the aftermath of the elections, sometimes we forget to put a face on the people who are living in more marginal circumstances – due to unemployment, etc.
We hear so much about fraud, waste and abuse of social programs that we forget about the real people who desperately need these services. Now, I am not some hippie advocating for radical political change.
I am just a nurse, trying to find the people who sometimes get forgotten in the middle of all this.
I am back in Mexicali (for the time being) but I was so busy during the last few weeks that I didn’t get to finish some of my posts talking about the interesting people I’ve met – and places I’ve seen.. I certainly don’t want to skip over Wilmer Villa.
He’s not famous, nor is he a surgeon – but just like so many of the people I’ve met in Colombia – he has a story to tell. It’ didn’t start as an interview, but then it rarely does – it started out as a visit to a salon on Calle 115 No 59 – 35 with a friend. But as Wilmer talked about his new salon (his first), and we celebrated the one month anniversary of his shoppe, a story started to form.
No, he hasn’t invented a cure for cancer – or even a way to arrest the relentless aging process. But he has managed to create a tranquil little spot in the middle of Bogotá for people to come and enjoy themselves for a few hours.
It hasn’t been easy – but with the help of a good friend (and long-time client), Alcira Acosta de Chaves, Wilmer was able to move out of the previous salon where he had a chair to establish his own salon. It’s a dream that has been several years in the making – which is obvious as soon as you enter the salon.
Everything is immaculate; organized and set out in a classically elegant black/white and silver scheme that evokes the 1940’s heyday of glamour. But it’s more than just a place for a haircut or a manicure, Wilmer. 27, states. It’s the entire package – the total experience, he explains, as he pours a client a cup of herbal tea.
“People can come here and get away from all the negative, and the stress [of their daily lives.] We are here for more than just hair, and make-up. we are here for laughter, smiles and good times with friends.
His cheerful attitude is infectious, and as clients come in, he and Almira take time to explain the philosophy of the shop, and the experience. “I want this place to be different” – it’s not a place for catty remarks, or cutting down of self-esteem. It’s not about malicious gossip or sarcasm, ” We don’t need any of that here,” he says. “It’s a place for people to form long-term relationships, share celebrations, milestones and happy events,” he adds. And he means it – as each person enters, he greets them by name, they share a smile or a silly story.
It’s nice – and certainly different from many of the other salons in the area. It isn’t about the up sell, or preying on women’s insecurities about their looks to sell services*. They seem to genuinely enjoy their customers and in making their clients look and feel their best.
About Wilmer:
Wilmer, the child of a Colombian mother and a Venezuelan father, was born Cucuta, near the border. He grew up in Chinacota, Colombia near the border with Venezuela. He attended cosmetology school in Perico before coming to Bogotá.
After finishing school, he come to Bogotá to apprentice with several well-known stylists such as Hernan Abandano, and received a scholarship for additional training as a colorist. He eventually received international certifications as a stylist and colorist – and has been a stylist for seven years.
He talks about how these experiences have shaped his life, and his outlook. “I like to meet people from different places, and hear more about their lives. I am learning English because I enjoy meeting and talking to Americans – and hearing their ideas and perspectives.”
Maybe Wilmer isn’t changing the world – but he is making it a more pleasant place.
*There is nothing more disheartening in my opinion than going for a manicure than being offered, “How about if we fix your hair” or “some Botox for those wrinkles”.. Or some other, more personal reminders that beauty, particularly in Latin America, is sometimes seen as more important that what’s inside.
Some of you have heard me talk about my friend, Jo O’shaughnessy before. She’s a fabulous photographer that I met here in Bogotá. (Told you there are always interesting and great people to encounter in this city.)
Jo has started a new blog, but she’s still getting the hang of it – so when she sent me one of her pictures of ‘Bogotá life’ – I told her I will be thrilled to share it. She is more than a photographer – she has the instincts and the artist sensibilities to see what other people overlook.
The next picture is a perfect example of that. On a rainy day in Bogotá – Jo looked out the window of a coffee shop and saw this man. He’s one of hundreds of scrap collectors in the city – people who make their living, and eek out a survival by collecting and reselling much of what the rest of the city regards as garbage. Like garbage, most people don’t even see the scrap collectors. They just become part of the city landscape, pulling their carts through traffic and enduring all sorts of conditions.
Few people stop to think about it. Fewer still can capture that daily struggle.
And then there’s Jo – whose heart is so big – and is practically chasing the man down the street to offer him her husband’s coat..
After a whirlwind three months that included trips to Chile, Bolivia and different cities in Colombia, I am getting ready to come home in a few days. As always, leaving Bogotá is bittersweet. I miss my friends, and my family but I will also miss the city and all of the nice people I’ve met here.
I am posting a map of Colombia, so even though I’ve taken several trips – you can see that I haven’t really explored the country at all. (I’ve posted little push pins on the areas I have visited.) I excluded Facativa and some of the closer towns since they are really just suburbs of Bogotá, and it would just clutter the map.
Map of Colombia, courtesy of Google Earth
As you can see – I haven’t explored the southern part of Colombia, or the pacific coast at all. My Atlantic adventures have been confined to Cartagena. So, I guess this means, I still have a lot of work cut out for me on my next visit(s).
map showing central Colombia
But I hope that readers have enjoyed reading about my travels, the people I’ve met and the things I’ve seen. Now – I know this is a medical/ surgery blog but since much of the surgery I write about is in this part of the world, I think that including some of my experiences is relevant/ interesting for people who read the blog. Once I get back home, I’ll post some more articles on medical quality control and standards – and more of my usual dry fare.
(Out of respect for patient privacy – I’ve done my best to crop the patient ‘bits’ from the photo.)
Spent some time last week with Dr. Alberto Martinez of Med-Sports Orthopedic Clinic here in Bogotá. Dr. Martinez specializes in arthroscopic surgery of the hips, knees and shoulders. As we talked about before, shoulder surgery is its own subspecialty in orthopedics due to the increased complexity of this joint.
We talked a bit about hip arthroscopy,which is still a relatively new procedure in orthopedics and the fact that one two surgeons in Bogota are currently performing this procedure.
Arthroscopy is the orthopedic minimally invasive counterpart to general surgery’s laparoscopy or thoracic surgery’s thoracoscopy. It involves insertion of a camera and several tools through small (1 cm) incisions in the skin. Arthroscopy itself has been used in orthopedics for many years but it is just now making inroads in hip procedures.
I’ll be publishing an upcoming article based on my observations over at ColombiaReports.com
After stuffing myself with lechona and tamal tolidense, swimming in the fresh crisp water of one of the local fincas, enjoying the controlled chaos of the market in Lerida and being overwhelmed by the tragedy of Armero – it was time to head back home to Bogotá.
Since it was Sunday, the roads were almost deserted, so we made it home in a fraction of the time it took to travel in the other direction. So much so, that we had plenty of time to stop and look around at more sites on the way home.
I got some great pictures of the drive – heading up into the cool mountains.
the valley below
One of the more interesting places we passed once we returned to Cundinamarca was Guaduas. Guaduas is a small city of about 30,000 that was the birthplace and home of one of Colombia’s most famous women (no, not Shakira but “La Pola”.)
The city was founded in 1572 and was a well-used and frequent stop for travelers from Bogotá to more outlying areas like Tolima. Now one of its main claims to fame is Policarpa Salavarrieta or “La Pola” as she is known. Her likeness and name currently adorn a local bakery in Guaduas.
Ms. Salavarrieta (1795 – 1817) is considered one of Colombia’s heroes (or heroine) for her role in the Colombian revolution. She is the only female to be honored on Colombian currency (in multiple different designations over the years.) She currently decorates the 10,000 peso bill, but was also on coinage in the past.
After being orphaned by a smallpox outbreak, she moved to Bogotá where she was able to sneak in and out of Bogotá (which had tight security under the Royalist regime).
She was a seamstress who used her sewing talents to gain access to the homes of staunch Royalists and eavesdrop on their conversations. She also stole documents and spied on military officers and recruited others to the revolutionary cause.
Unfortunately, after the capture of one of her fellow revolutionaries, she was arrested, tried and executed along with her lover and several others on November 14, 1817. She was reportedly defiant even as she was led to the firing squad, and refused to keep her back to her executioners – turning around to face them as they shot her to death.
To commemorate her actions to assist the revolutionary efforts, in the late 1960’s, the Colombian government designated her birthday as “Day of the Colombian Woman.”
After learning more about La Pola from my guide, we continued to Faca (Facativa), a city just outside Bogotá to visit one of the fincas that used to be in the family. Faca is best known for its native roots, and the many indigenous carvings, paintings and sculptures that were found during archeological excavations. Faca is primarily a farm town – and is surrounded by several large fincas with livestock and different agricultural products including flower cultivation.
From there – we cruised on into Bogotá; where as much as I enjoyed my journeys, it felt great to be home.
“Nocturno”
Oh dulce niña pálida, que como un montón de oro
de tu inocencia cándida conservas el tesoro;
a quien los más audaces, en locos devaneos
jamás se han acercado con carnales deseos;
tú, que adivinar dejas inocencias extrañas
en tus ojos velados por sedosas pestañas,
y en cuyos dulces labios —abiertos sólo al rezo—
jamás se habrá posado ni la sombra de un beso…
Dime quedo, en secreto, al oído, muy paso,
con esa voz que tiene suavidades de raso:
si entrevieras en sueños a aquél con quien tú sueñas
tras las horas de baile rápidas y risueñas,
y sintieras sus labios anidarse en tu boca
y recorrer tu cuerpo, y en su lascivia loca
besar todos sus pliegues de tibio aroma llenos
y las rígidas puntas rosadas de tus senos;
si en los locos, ardientes y profundos abrazos
agonizar soñaras de placer en sus brazos,
por aquel de quien eres todas las alegrías,
¡oh dulce niña pálida!, di, ¿te resistirías?…
The poem is actual microprinted on the reverse side of the 5,000 peso bill but despite using my macrolens – it’s impossible to read – I can’t even verify exactly which version is printed here, though one of my sources says Nocturno III, the rest just say Nocturne. But the bill itself is pretty impressive.
Una noche
Una noche toda llena de perfumes, de murmullos y de músicas de alas,
Una noche
En que ardían en la sombra nupcial y húmeda las luciérnagas fantásticas,
A mi lado lentamente, contra mí ceñida toda, muda y pálida,
Como si un presentimiento de amarguras infinitas,
Hasta el más secreto fondo de las fibras te agitara,
Por la senda florecida que atraviesa la llanura
Caminabas,
Y la luna llena
Por los cielos azulosos, infinitos y profundos esparcía su luz blanca,
Y tu sombra
Fina y lánguida,
Y mi sombra
Por los rayos de la luna proyectadas,
Sobre las arenas tristes
De la senda se juntaban,
Y eran una,
Y eran una,
Y eran una sola sombra larga
Y eran una sola sombra larga
Y eran una sola sombra larga…
Esta noche
Solo; el alma
Llena de las infinitas amarguras y agonías de tu muerte,
Separado de ti misma por el tiempo, por la tumba y la distancia,
Por el infinito negro
Donde nuestra voz no alcanza,
Mudo y solo
Por la senda caminaba…
Y se oían los ladridos de los perros a la luna,
A la luna pálida,
Y el chillido
De las ranas…
Sentí frío; era el frío que tenían en tu alcoba
Tus mejillas y tus sienes y tus manos adoradas,
Entre las blancuras níveas
De las mortuorias sábanas,
Era el frío del sepulcro, era el hielo de la muerte
Era el frío de la nada,
Y mi sombra,
Por los rayos de la luna proyectada,
Iba sola,
Iba sola,
Iba sola por la estepa solitaria
Y tu sombra esbelta y ágil
Fina y lánguida,
Como en esa noche tibia de la muerta primavera,
Como en esa noche llena de murmullos de perfumes y de músicas de alas,
Se acercó y marchó con ella
Se acercó y marchó con ella…
Se acercó y marchó con ella…¡Oh las sombras enlazadas!
¡Oh las sombras de los cuerpos que se juntan con
[las sombras de las almas…
¡Oh las sombras que se buscan en las noches de tristezas y de lágrimas!..
microscript
Earlier, I posted what was supposed to be an ‘official translation’ but even as I compared the two – with my limited Spanish – it seemed really, really off. (Not just shades of nuance – which I have yet to master in Spanish.)
Jose Asuncion Silva (1865 – 1896)
They say that Jose Asuncion Silva wrote those words after the death of his beloved sister in 1892, but reading his words more than a century later – I have my doubts. Unless, like Poe, he nurtured a romantic love for a close family member (Poe married his first cousin.)**
Otherwise, to me – the words speak of a more romantic, more tragic love with a lot of sensual imagery, but of course, that is just my interpretation of my modest Spanish, as well as google translation.
A few years after his sister’s death, the majority of his work was lost at sea (1895). Shortly after, in 1896 – burdened by family debt and these emotional losses – Jose Asuncion Silva committed suicide by shooting himself in the chest.
His most famous work – (as posted above) wasn’t published until well after his death in 1908.
You can visit his grave at the Central cemetary here in Bogotá. (The link is to one of my favorite Bogotá bloggers). ** Local rumor is that he did, indeed, harbor an ‘unnatural affection for his dear sis..
He lives at the top of the world, I think as I climb the hills of Bogota to his studio. In a sliver of the window of his modest work space, the whole of Bogota is laid out beneath me. I wonder how this affects the Bogota native’s work; which is dark, profound and futuristic in nature.
Film Director, Andres Barrientos
In a city where chance meetings are common, I had the good fortune to sit next to a charming and attractive young man at a friend’s dinner party. As we made the usual small talk, he mentioned that he was a filmmaker.
Now, growing up in California, I had met my share of ‘filmmakers,’ all of who were the self-proclaimed ‘next Scorsese’ or ‘Tarentino’, and all of whom were waiting tables. So we talked about YouTube and the like, along with one of his current projects, while I remained mainly grateful for the timely rescue his appearance made from the boorish oaf on the other side of me. He was interesting and charming enough that I offered to interview for him for my modest little blog.
Imagine my surprise to find out that he’s not the next Clint Eastwood. Or even Tarentino. No, he’s theAndres Barrientos, one of Colombia’s youngest critically acclaimed directors with over fifteen films (and numerous awards) to his credit. Despite my appalling lapse, he was delightful, kind and prompt. (The last is especially notable in Colombia, where time has its own interpretation.)
Andres Barrientos, working in his studio
It will take several days to unravel the complexities of Mr. Barrientos and his work – but I’ll be talking more about him and the three projects he is currently working on over at the Examiner.com.
Like I’ve said in a previous post – one of the great things about living in a city like Bogotá, is all of the interesting people.. Some of them are lifelong residents, some are visitors like myself – and others are making Bogotá a temporary home, like my friend, Johanna and her husband, Paul.
a true photographer, my friend, Johanna
Johanna’s a talented photographer (I’ve much admired her photos for a long time) so I am hoping to enlist her in some of my efforts.. She took several of the pictures here (the good ones!)
Yesterday, we went to La Calera which is a picturesque community just outside of the city. Sundays are a particularly popular day for city residents to get a taste of small town life just twenty minutes outside Bogotá.
leaving the rainy city behind for a day in La Calera
But our excursion yesterday was a bit different from some of the lovely, and lazy afternoons I’ve had wandering the villages surrounding Bogotá. This time, we were there for a cause.
nope, still not in trouble.. just hanging out
We joined Colombia’s Civil Defense – Cundinamarca division for a toy drive to benefit children in one of the outlying villages.
Civil Defense 4 x 4 division toy drive
They will deliver the toys by 4 X 4 next month..
with the Colombia’s Civil Defense
While they were collecting toys – they also had some activities for the local kids – including a ‘Paint the Car’ activity which proved popular with kids and adults alike. (After all – how often do the police hand out spray paint?)
Civil defense officer helps a small child paint
It was a lot of fun – for a good cause, so I’ve written some more about it over at Examiner.com.
Hoping to do some more interviews this week – to bring more of Bogotá’s residents to readers..
After a year and a half – it was time to stop in at Santa Fe de Bogotá and see what was new.
Dr. Roosevelt Farjardo, MD (general surgeon) has been instrumental in implementing some of these new and exciting changes such as the ‘Virtual Hospital’ that I will be writing about (soon). He was very nice about taking time to update me on some of his new programs at part of the Center for innovation in education and health. Telemedicine is just the tip of the iceberg as far as some of the cool things they are doing.
Unfortunately, the same can’t be said of the International Patient Center – or rather – I can’t report anything other than the fact that Ana Maria Gonzalez (the previous director) has left for a position in the United States and that Dr. Carolina Munoz has taken her place.
I was hoping to get some statistics and report back about some of the specialty programs for overseas travelers – but Alas! I am unable to bring this information to you. I waited over 70 minutes after my scheduled appointment with Dr. Munoz – and despite several calls from her staff, she never showed up and never attempted to reschedule.
I wish I could say this is an isolated incident – but I am afraid this is more like a clash of “cultures”. I say this because I met with Dr. Munoz previously; during the writing of the book (when she was the Director of the International Patient Center at rival Fundacion Cardioinfantil.)
At that time, (if I remember correctly, she introduced herself as a cardiac surgeon who had retired to “spend more time with her children.”)
Of course, my obvious question – was “oh, and how many children do you have?**”
I thought we were making polite conversation – because at the time, I was less familiar with Colombian customs, culture etc. In reality, she was reminding me of her elevated stature in comparison to mine (as ‘just a nurse’). Dense as I was – it became obvious as the interview progressed – as she made sure that I knew that she had replaced her rival (Ms. Ana Maria Gonzalez – RN) who had also worked at Fundacion Cardioinfantil in the past. I’m sure she resented having to answer questions about the Executive Health Program and other aspects of their medical tourism program from someone she found to be inferior to herself. (She made that pretty clear at that initial interview back in 2011).
So I guess it is no surprise that she didn’t bother to show up to our appointment this week – which is a shame, as I had looked forward to finding out more about the evolving International Patient Center at Santa Fe de Bogotá.
Luckily for me – there was another nurse there, Sandra Salazar – who could give me some basics. She was delightful, helpful and dreadfully embarrassed about the whole thing. She was even able to give me a list of some of the American insurance companies they have worked with in the past. I had lots of questions about the HIPEC program, which she couldn’t answer – but she outlined the entire medical tourist process – and answered a lot of other questions. She showed me how they streamline the process for their international patients, and the process for medical and surgical evaluations.
Now, there’s some good news for readers: You aren’t nurses. You are paying customers – so I am sure that Dr. Carolina Munoz will put aside any of her personal feelings (whatever they are) towards foreigners and will make time for you.
**The answer as none – as she is not married, and was not planning to be married in the foreseeable future.
Now when I am talking about culture – I am not strictly talking Colombia – America. I am talking about Doctor – Nurse relations. Watch some old Turner Classic Movies sometime and you will see what I mean..
Now I debated writing about this, but after talking with some other non-Colombians here in Bogotá, I felt it was important to pass it along because it illustrates quite a few things about my work:
1. It’s not as easy as it looks (I spend a huge amount of time waiting..)
2. Cultural differences can cause a lot of problems – so be prepared to be tolerant.
3. If there is a chance that patients may get poor service – I want to know about it! (And part of readers need to know about – is my experiences.)
Just a few more weeks here in Bogotá before heading back to the United States. My days are crammed with interviews – so I haven’t been posting as much as usual.
Right now, I am making copious notes – and taking plenty of photos so I can starting writing up several articles in the next several weeks. Much of my work will be published over at Colombia Reports.com so I will attempt to keep from duplicating it here. (Also – I won’t have the time..)
I’ll still try to post pictures and stories here – about Bogotá life in general, to give readers a sense of the city, and the people here since that’s something that they won’t get with my (rather) dry surgical descriptions/ evaluations.
But – I am already working on plans to return to Bogotá, (and other parts of Colombia) this spring. Once I have some concrete plans, I’ll post them here for readers and (potential travelers..)
homeless in Bogotá
I wandered around Avenue Caracas (Carrera 14) for a bit this afternoon. It’s not the best area because there are a lot of homeless people, and it has a reputation for quite a bit of crime (muggings and such) but I couldn’t resist walking by the “Calle de Mascotas” or the three blocks (from Calle 53-56) on Avenue Caracas that hold about a dozen pet stores..
The man crouched down in the photo above just finished stamping out his cooking fire as I came by..
kittens in a pet shop window
It was particularly heart-wrenching for me – while I’ve been down here in Bogotá, my long-time friend and companion – my 17-year-old cat passed away. (Don’t worry, he was surrounded by loved ones, and died in my husband’s arms).
This inquisitive little fellow here reminded me quite of a bit of my cat (though they do not look-alike.) So it was hard to keep walking – but then next to one of the pet stores, I watched two artists create this mural..
a work in progress
Hard to believe all this detail came from spray paint (no brushes!) but it did..
working on the mural
This artist, and his assistance were really nice, and didn’t mind me taking their pictures.
Interview at noon today with Traveling for Health – where you can call in and ask questions.. You can find the show here. Don’t worry, if you miss it – you can hear it in the archives next week.